
Mastering the Elbow Exam: A Step-by-Step Guide for Chiropractors
Elbow pain is one of the most common upper extremity complaints in clinical practice, yet it’s frequently misdiagnosed. While many cases are labeled “tennis elbow,” a significant portion involve nerve entrapments or referred pain that require a more precise approach.
This blog features a comprehensive elbow physical exam tutorial to help you elevate your diagnostic skills to the next level! In the next few minutes, you’ll review:
A 2-minute elbow exam you can use immediately
The most accurate tests for lateral and medial epicondylopathy
When imaging is helpful…and when it’s not
Watch this micro-webinar on performing an elbow physical exam.
1. What Are the Most Common Causes of Elbow Pain?
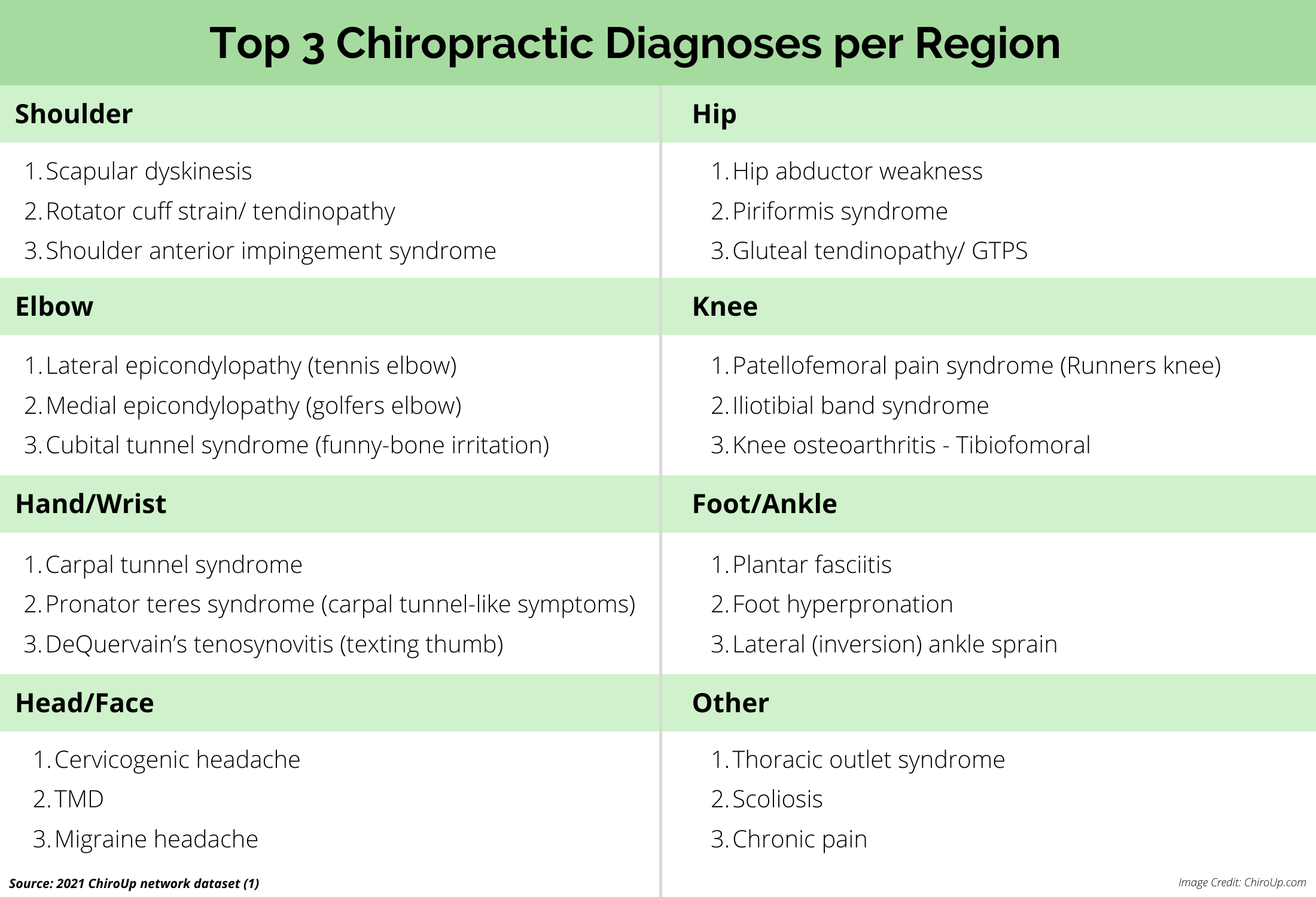
According to the ChiroUp Network Dataset Analysis of 631,970 clinical diagnoses collected from more than 2,200 evidence-based chiropractic providers, the top three most common elbow diagnoses in chiropractic offices were:
Lateral epicondylopathy
Medial epicondylopathy
Cubital tunnel syndrome
2. Elbow Pain Differential Diagnosis
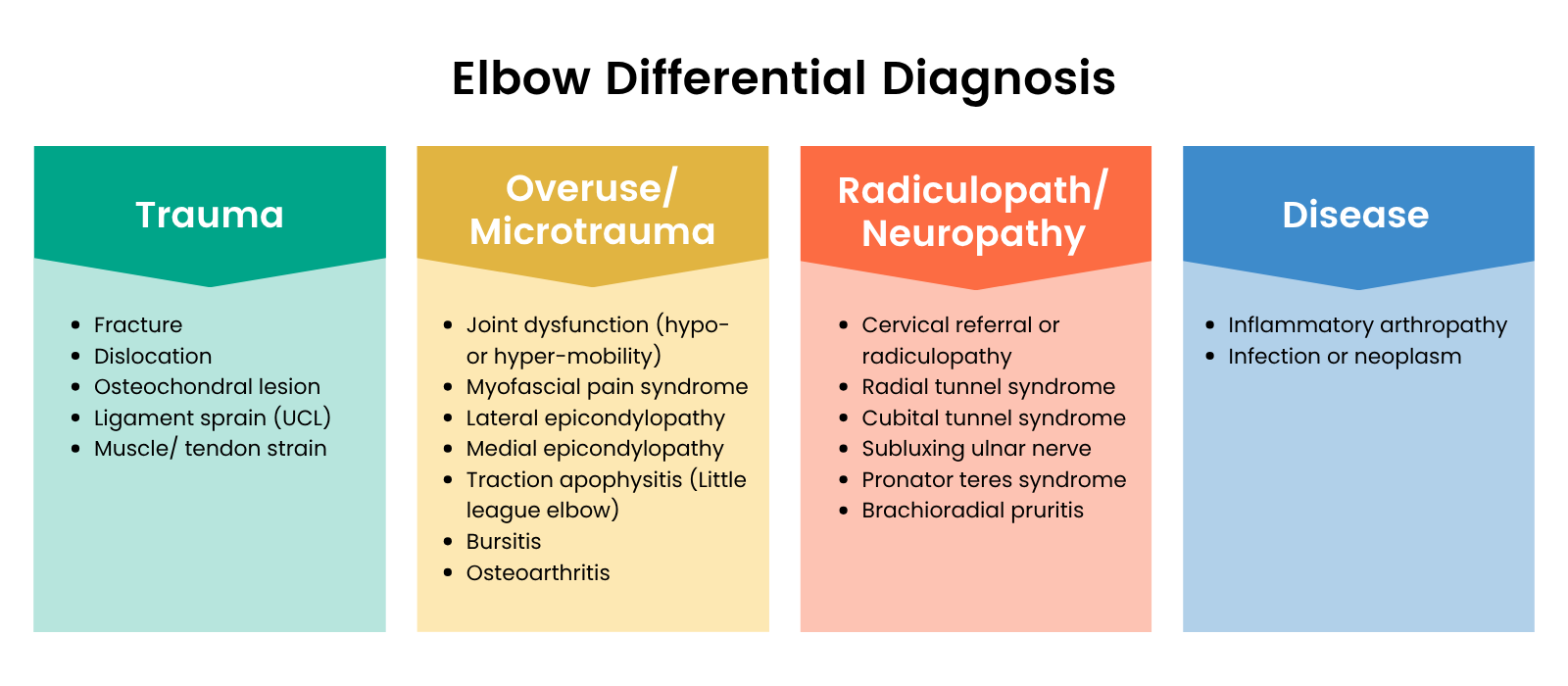
Before jumping into testing, it’s critical to understand the full range of potential elbow pain diagnoses. In addition to the common culprits listed above, providers must consider many other potential diagnoses affecting the region's bones, joints, cartilage, ligaments, tendons, muscles, and nerves.
An expanded elbow differential diagnosis should include:
3. Essential Questions To Ask During an Elbow Exam
Once you’ve considered the differential, your history becomes the most powerful diagnostic tool. Key history questions during an elbow physical exam include:
🔹 Onset- Traumatic onset of elbow pain may indicate conditions such as fracture, dislocation, ligament injury, or muscle/tendon strain. Conversely, non-traumatic elbow pain often develops gradually and is more commonly associated with overuse conditions such as lateral or medial epicondylopathy, nerve entrapments, or degenerative changes. Repetitive loading activities, including gripping, lifting, throwing, or prolonged elbow positioning, are frequently responsible for microtrauma that drives these conditions.
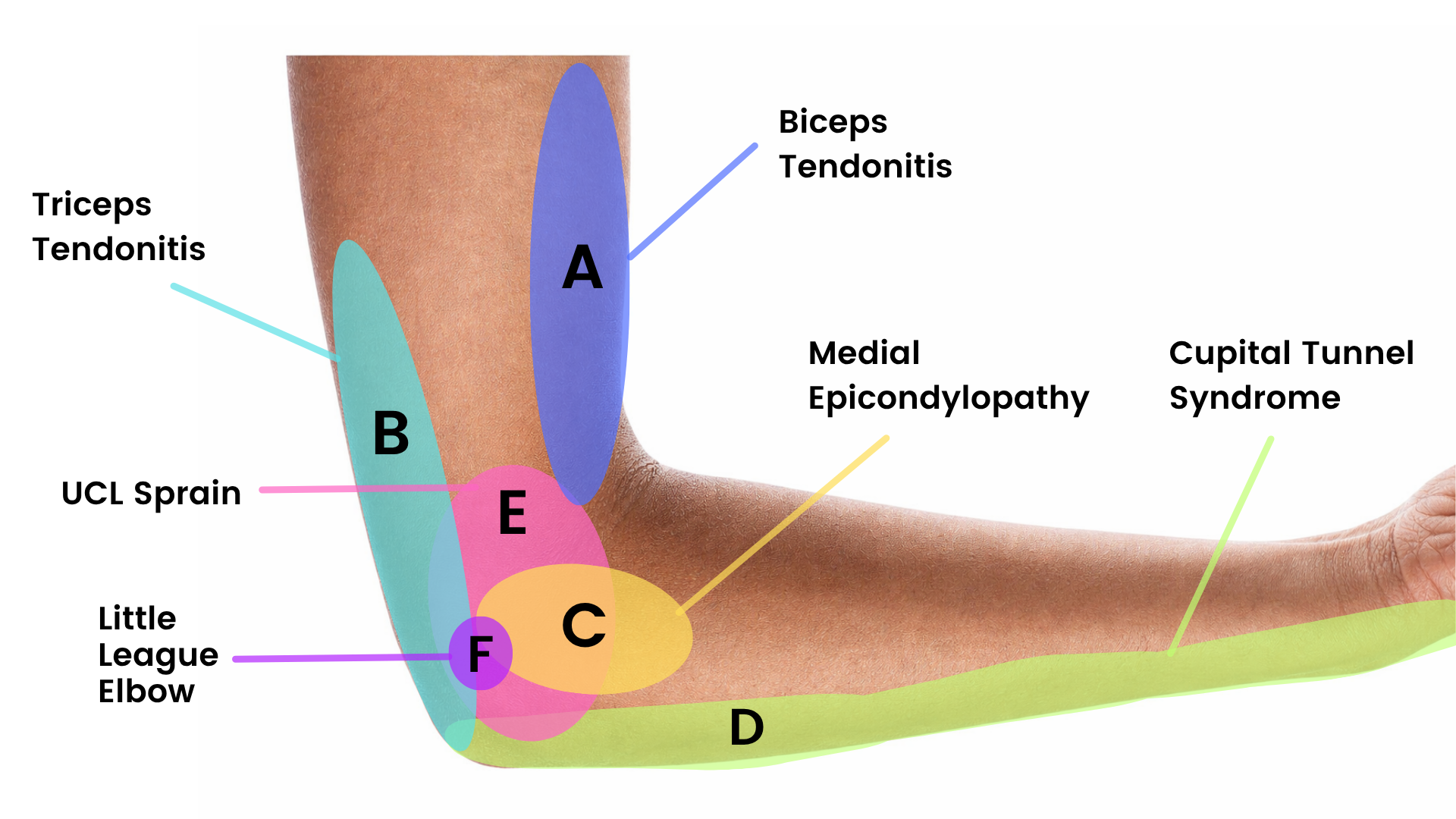
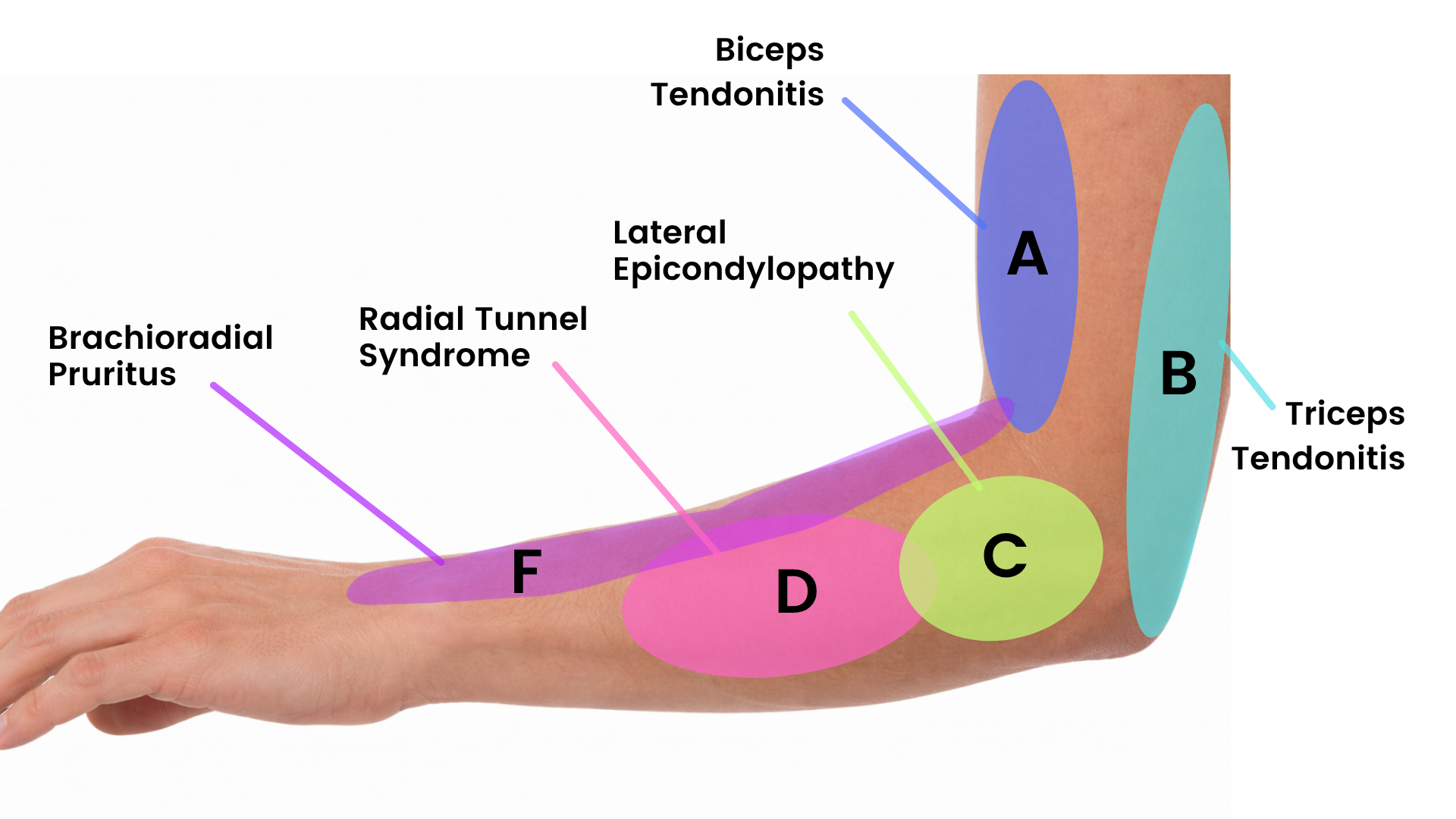
🔹 Symptom Location and Character- Pain location can provide valuable diagnostic insight, although several elbow conditions share overlapping referral patterns.
🔹 Aggravating Activities- Pain with gripping or resisted wrist extension is strongly associated with lateral epicondylopathy, while discomfort with wrist flexion or pronation more commonly suggests medial epicondylopathy. Symptoms provoked by sustained elbow flexion, such as holding a phone or sleeping with the elbow bent, are characteristic of cubital tunnel syndrome. Pain reproduced during forearm resisted supination may indicate radial tunnel syndrome.
🔹 Stiffness and Mechanical Symptoms- Morning stiffness may indicate underlying osteoarthritis or inflammatory conditions, particularly if stiffness persists beyond typical activity-related soreness. Mechanical symptoms such as locking, catching, or an inability to fully extend the elbow may suggest intra-articular pathology, including loose bodies or osteochondral lesions. Progressive loss of motion is more commonly associated with chronic or degenerative joint conditions.
🔹 Age- In children and adolescents, clinicians should consider growth-related conditions such as Little League elbow, where repetitive valgus stress affects the developing medial elbow. In adults, epicondylopathy and nerve entrapments are more common, while older individuals are more likely to present with osteoarthritis.
🔹 Health History- Conditions such as diabetes increase the risk of peripheral neuropathy, while metabolic or endocrine disorders may contribute to tendon degeneration. Rheumatologic diseases should also be considered in patients presenting with bilateral symptoms, prolonged stiffness, or systemic complaints.
Deeper dive: ChiroUp subscribers can download our Inflammatory Arthropathy Infographic from the Forms Library. Just go to Practice Resources > Forms Library and search “arthropathy”.

4. How to Perform an Elbow Exam
The essential components of a physical exam for elbow pain include:
Inspection - swelling, deformity, atrophy
Range of motion - active, passive, and resisted movements
General palpation - tenderness, swelling, and warmth
Joint palpation - stability testing, motion palpation
Orthopedic assessment - various elbow orthopedic exam tests specific to the differential diagnoses
Functional assessments - scapular dyskinesis, upper crossed syndrome, etc.
Neuro eval - sensory disturbances/ dermatomes, myotomes, reflexes, plus neurodynamic assessments/ nerve tension tests.
For a Deeper dive, check out our most popular chiropractic blog detailing 3 simple Nerve Flossing Exercises for Arm Pain.
Cervical evaluation: radiculopathies often refer to the elbow, and nearly four out of ten elbow problems may arise from an asymptomatic spine. (1)

5. Key Elbow Diagnoses You Must Identify
Lateral Epicondylopathy
The most common cause of elbow pain, affecting 1–3% of the population annually. (2,3)
Degenerative condition of the extensor carpi radialis brevis
Pain with gripping and wrist extension
Localized tenderness at the lateral epicondyle
Key tests for lateral epicondylopathy:

Cozen’s Test

Mill’s Test
Radial Tunnel Syndrome
Radial tunnel syndrome frequently mimics lateral epicondylopathy, but requires a different treatment approach. The condition is often caused by irritation of the radial nerve as it passes beneath the supinator muscle.
Pain is more distal and diffuse
Often worse at night
May include sensory or motor findings (i.e., finger drop)
Key tests for radial tunnel syndrome:

Radial Tunnel Compression Test

Resisted Middle Finger Extension
Deeper Dive: Check out our blog on lateral epicondylopathy vs radial tunnel syndrome.
Medial Epicondylopathy
3–10x less common than lateral epicondylopathy (4,5,6)
Pain with wrist flexion and pronation
Often associated with valgus stress
Key tests for medial epicondylopathy:

Golfer’s Elbow Test

Resisted Forearm Pronation
Cubital Tunnel Syndrome
The second most common compressive neuropathy after carpal tunnel syndrome (7,8)
Paresthesia in the 4th and 5th digits
Nocturnal symptoms are common
Progressive weakness in advanced cases
Key tests for cubital tunnel syndrome:

Ulnar Nerve Self Test

Tinel’s Sign
Two Hidden Diagnoses You Don’t Want to Miss
Two commonly overlooked conditions can masquerade as more routine elbow complaints and persist if not identified early. We’ve covered each of these commonly overlooked diagnoses in more detail in prior blogs. Be sure to check those out if you want a deeper dive.

Brachioradial Pruritus
Brachioradial pruritus is a commonly overlooked neuropathic condition that causes itching, burning, or tingling along the lateral forearm, often without visible skin changes. It is frequently linked to cervical nerve irritation rather than a primary skin problem.
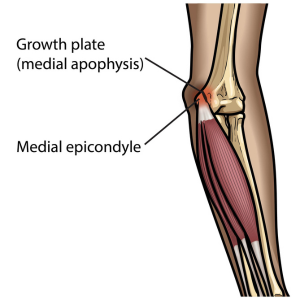
Little League Elbow
Little League elbow is an overuse injury of the medial elbow in skeletally immature athletes, most often caused by repetitive throwing. Early recognition is important because the underlying problem is often growth plate stress rather than simple tendon irritation.
Turn Your Diagnosis Into a Finished Note in Seconds
5. When to Image the Elbow
Most elbow pain does not require imaging. However, when indicated, the American College of Radiology (ACR) recommends radiographs as the initial imaging study for both acute and chronic elbow pain. (9,10) Use X-rays first when:
Trauma is present
Pain is persistent or unclear
Mechanical symptoms are reported (locking, catching)
If X-rays are negative, further imaging should be based on clinical suspicion:
Suspected fracture (occult) → Repeat X-ray (10–14 days) or CT
Suspected tendon or ligament injury → Ultrasound or MRI
Persistent epicondylopathy not improving with care → Ultrasound or MRI
Mechanical symptoms (locking, catching) → MRI or CT (± arthrogram)
Suspected nerve involvement → Ultrasound or MRI
Clinical takeaway: Start with X-ray. Escalate based on what you suspect, not just pain. And remember that imaging findings often do not correlate with symptoms, especially in tendinopathy.
Final Thoughts: Mastering the Elbow Exam
Mastering the elbow exam doesn’t require complexity; it requires clarity. By combining a focused history, pattern recognition, and a handful of high-yield tests, clinicians can quickly differentiate between tendinopathy, nerve entrapment, and referred pain.
Use this elbow pain diagnostic flowchart as a quick clinical guide to streamline your exam and improve diagnostic accuracy in seconds.
Continue Mastering Regional Exams
Looking to sharpen your exam skills across the entire body? Explore our complete series of regional exam guides below:
Elbow Exam FAQ
-
Lateral epicondylopathy is the most common cause, particularly in patients with repetitive gripping activities.
-
Lateral epicondylopathy presents with localized pain at the lateral epicondyle, while radial tunnel syndrome causes more diffuse, distal pain and is often worse at night.
-
Imaging is indicated for trauma, persistent symptoms, mechanical dysfunction, or suspected structural pathology. X-rays are the first-line study. (9,10)
-
Yes. Up to 40% of elbow pain may originate from the cervical spine, even without obvious neck symptoms. (1)
Now that you’ve got the lowdown on the essential tests for diagnosing elbow pain, it’s time to take that knowledge and run with it. ChiroUp subscribers can dive into the Clinical Skills tab for step-by-step tutorials on best-practice treatments, exercises, and ADL advice your patients need.
-
1. Rosedale R, Rastogi R, Kidd J, Lynch G, Supp G, Robbins SM. A study exploring the prevalence of Extremity Pain of Spinal Source (EXPOSS). Journal of Manual & Manipulative Therapy. 2020 Aug 7;28(4):222-30. Link
2. Bigorre N, Raimbeau G, Fouque PA, Saint Cast Y, Rabarin F, Cesari B. Lateral epicondylitis treatment by extensor carpi radialis fasciotomy and radial nerve decompression: Is outcome influenced by the occupational disease compensation aspect?. Orthopaedics & Traumatology: Surgery & Research. 2011 Apr 1;97(2):159-63. Link
3. Hong QN, Durand MJ, Loisel P. Treatment of lateral epicondylitis: where is the evidence?. Joint Bone Spine. 2004 Sep 1;71(5):369-73. Link
4. Shiri R, Viikari-Juntura E, Varonen H, Heliövaara M. Prevalence and determinants of lateral and medial epicondylitis: a population study. American journal of epidemiology. 2006 Dec 1;164(11):1065-74. Link
5. Polkinghorn BS. A novel method for assessing elbow pain resulting from epicondylitis. Journal of chiropractic medicine. 2002 Jun 1;1(3):117-21. Link
6. McHardy A, Pollard H, Luo K. Golf injuries. Sports Medicine. 2006 Feb 1;36(2):171-87. Link
7. Cutts S. Cubital tunnel syndrome. Postgraduate medical journal. 2007 Jan 1;83(975):28-31. Link
8. Chauhan M, Anand P, Das JM. Cubital Tunnel Syndrome. StatPearls [Internet]. 2020 Mar 24.Link
9. American College of Radiology. ACR Appropriateness Criteria. Acute Elbow and Forearm Pain. Reston (VA): American College of Radiology; 2022. Link
10. American College of Radiology. ACR Appropriateness Criteria. Chronic Elbow Pain. Reston (VA): American College of Radiology; 2018. Link