
Chiropractic E/M Coding Guide Part 1: New vs. Established Patients (99202–99215 Explained)
A patient walks into your clinic with acute low back pain. You evaluate, adjust, and document appropriately—but then pause: Is this a 99203 or a 99213? That single decision can mean the difference between proper reimbursement and audit risk.
Accurately coding Evaluation and Management (E/M) visits is essential for chiropractors. Correct coding ensures compliance, supports reimbursement, and strengthens patient documentation. A common area of confusion is distinguishing between new and established patients, which directly affects coding, documentation, and payer audit risk.
In this first part of a four-part series, Dr. Evan Gwilliam, Senior Vice President at Practisync, breaks down the practical differences and provides actionable guidance for coding new vs. established patients.
E/M Coding for New Chiropractic Patients
A new patient is someone who has not received professional services from you or another chiropractor in the same group in the past three years.
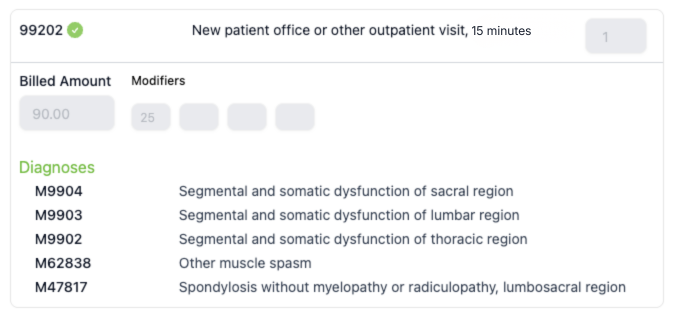
New patient visits generally require a more thorough history and exam and involve more complex medical decision-making (MDM) than a typical office/outpatient established patient E/M service. The new patient codes cover time ranges from 15 to 74 minutes and levels of decision-making from straightforward to high. Even if the visit focuses on manual therapy, proper documentation of evaluation and assessment is critical to justify the E/M level. Office/outpatient CPT codes for new patients fall in the 99202–99205 range, with 99202 and 99203 being the most frequently used in chiropractic.
E/M Coding for Established Chiropractic Patients
Unlike new patients, an established patient has been seen at your clinic within the past 3 years by you or a provider in your specialty.
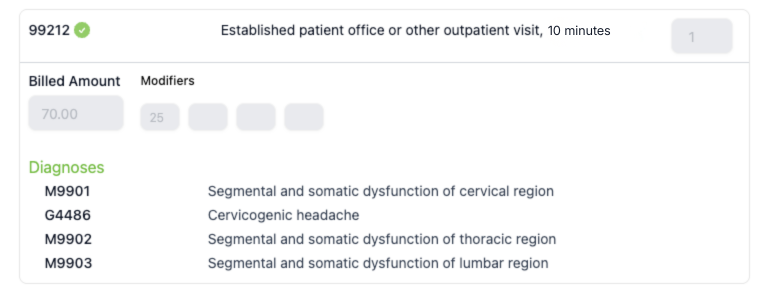
Documentation for these visits, if a re-exam, should focus on changes since the initial exam, including updates to the patient’s history, response to treatment, and plan-of-care adjustments. MDM may be less complicated than new patient encounters, and the visits may be shorter. The codes for office/outpatient established patient encounters include a time range from 10 to 54 minutes and MDM from straightforward to high (99212-99215). In chiropractic practice, the most commonly used codes for these visits are 99212 and 99213.
Quick Reference: New vs. Established Patient E/M Coding
| New Patient | Established Patient | |
|---|---|---|
| Definition | Not seen in the past 3 years by you or another provider in the same group/specialty | Seen within the past 3 years by you or another provider in the same group/specialty |
| Complexity (MDM) | Straightforward – High | Straightforward – High |
| Encounter Time | 15–74 min | 10–54 min |
| Common CPT Codes | 99202–99205 (Most common: 99202–99203) | 99211–99215 (Most common: 99212–99213) |
*Audit risk: Payers frequently audit E/M codes due to inconsistent documentation, especially when higher-level codes are used without clear medical necessity.
2021 E/M Coding Updates: What Chiropractors Need to Know
The E/M coding guidelines were significantly overhauled in 2021, with minor updates in 2023 and 2024. The goal, according to the AMA, was to focus documentation on how providers think and care for patients rather than rigid checklists:
“…documentation for E/M office visits will now be centered around how physicians think and take care of patients and not on mandatory standards that encouraged copy/paste and checking boxes.” (1)
The changes were designed to simplify documentation, reduce note bloat, and allow providers to focus more on patient care. The most important principle remains medical necessity. Code selection should reflect the complexity of the patient’s condition—not just whether the notes include all guideline elements.
The biggest change in 2021 was the removal of History and Examination as factors for determining the E/M level. Instead, code selection now depends on medical decision-making (MDM) or the total time spent performing the service. These topics will be explored in more detail in parts 2, 3, and 4 of this series.
FAQs
-
A patient is considered established if they’ve received professional services from you or another provider in your clinic group within the past 3 years. If not, they are considered a new patient.
-
No. If the provider is part of the same clinic group and shares the same specialty, the patient is still considered established.
-
No. Patient status is based on the provider relationship within the past 3 years, not the condition being treated.
Conclusion
Accurately distinguishing between new and established patients is key for proper E/M coding. Chiropractors should verify patient status, tailor documentation to the visit type, and fully capture history, exam, and medical decision-making.
Want to eliminate E/M coding guesswork? ChiroUp’s EHR helps guide documentation and coding based on clinical inputs, helping you stay compliant and efficient. See how it works in a quick walk-through with our team.
This is Part 1 of a 4-part E/M Coding Mastery Series. Stay tuned for the following parts to be released over the next few months:
Part 2: Medically Appropriate History and Examination
Part 3: Coding Using Time
Part 4: Coding Based on Medical Decision Making
-
American Medical Association. CPT® evaluation and management. American Medical Association. Link