
Joint Hypermobility Syndrome and Hypermobility Spectrum Disorder: Chiropractic Diagnosis and Treatment
A young patient presents with chronic neck and low-back pain that has persisted for years. Imaging is unremarkable. Manipulation provides temporary relief, but the pain quickly returns. The patient mentions that they were “double-jointed” as a child and frequently sprained their ankles while playing sports.
Situations like this are surprisingly common. Generalized joint hypermobility, once dismissed as a benign trait, has increasingly been recognized as a significant contributor to chronic musculoskeletal complaints. Many hypermobile patients experience persistent pain, fatigue, and recurrent injuries, yet the condition often goes undiagnosed for years. (1)
For chiropractors, recognizing the hypermobile patient can fundamentally change management. Traditional mobility-focused care may provide short-term relief but fail to address the underlying problem: insufficient joint stability.
This blog explores how chiropractors can recognize joint hypermobility and hypermobility spectrum disorders, understand their clinical presentation, and apply evidence-based conservative management strategies.
1. What Is Joint Hypermobility?
Joint hypermobility refers to joints that move beyond the normal expected range of motion due to ligamentous laxity and connective tissue differences. While some individuals are asymptomatic, others develop hypermobility spectrum disorders (HSD) characterized by chronic musculoskeletal pain, joint instability, fatigue, and recurrent injuries. Diagnosis commonly involves clinical screening tools such as the Beighton score and the Hakim and Grahame questionnaire.
Joint hypermobility is best viewed as a descriptive finding rather than a diagnosis and may reflect an underlying connective tissue disorder. (2) Modern classification systems recognize symptomatic hypermobility as part of a continuum known as the hypermobility spectrum. (3)
The Hypermobility Spectrum
| Diagnostic Term | Clinical Distinction | Diagnostic Requirement |
|---|---|---|
| Generalized Joint Hypermobility | An asymptomatic physical trait describing excessive ROM in multiple body regions. | Positive Beighton Score (age-dependent cut-offs). |
| Hypermobility Spectrum Disorder | Symptomatic hypermobility that does not meet strict Ehlers-Danlos criteria. | Symptomatic joint hypermobility with exclusion of Ehlers-Danlos and related syndromes. |
| Hypermobile Ehlers-Danlos Syndrome | A systemic heritable connective tissue disorder with musculoskeletal and extra-articular features. | Generalized Joint hypermobility, systemic features, and family history with exclusion of other connective-tissue disorders. |
2. How Common Is Hypermobility?
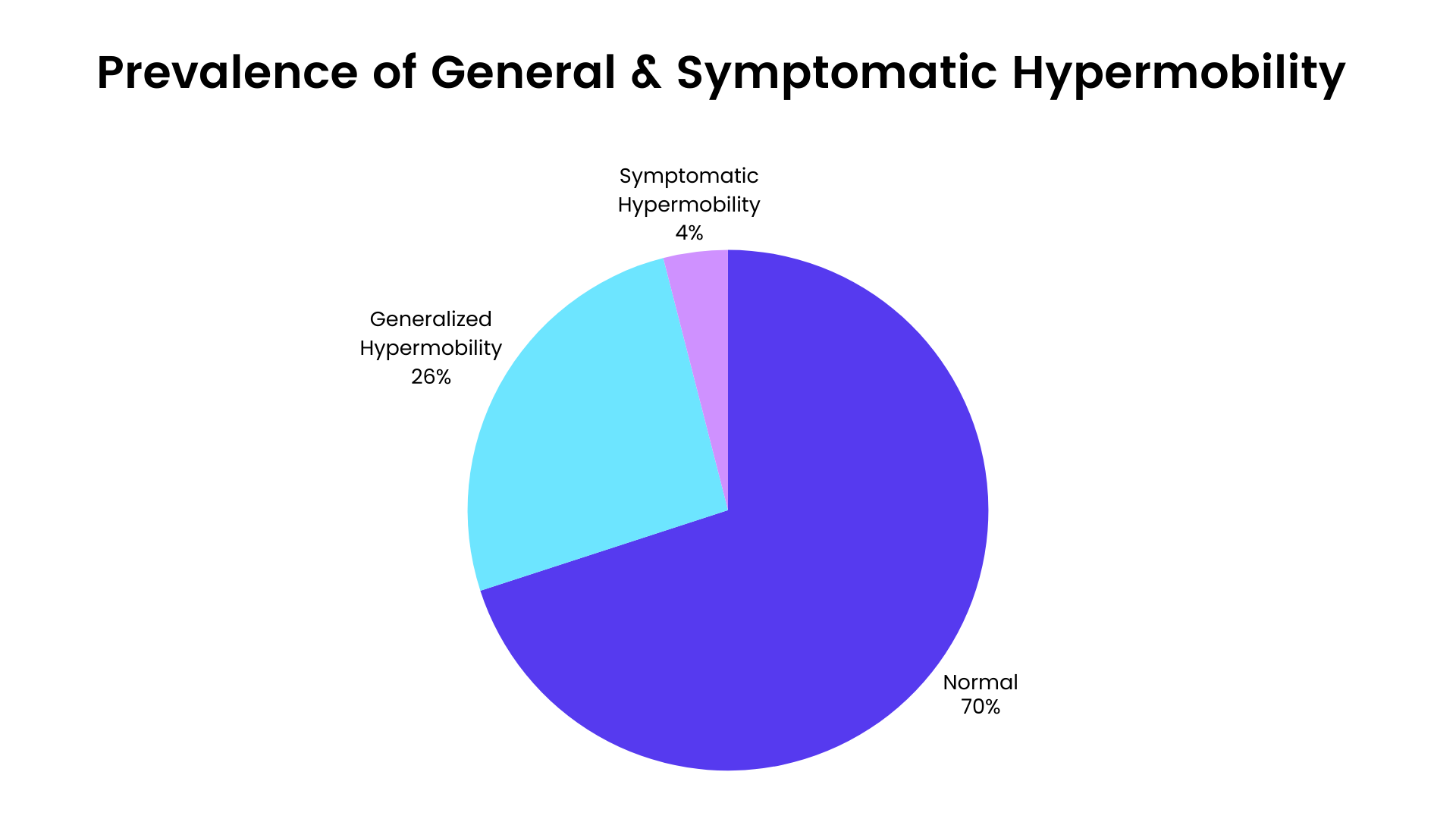
Joint hypermobility is far more common than many clinicians realize. Estimates suggest that 10–30% of the general population may demonstrate joint hypermobility traits. (4,5 )
Only a subset of individuals with joint hypermobility develop symptomatic hypermobility spectrum disorders, which are estimated to affect roughly 1–4% of the population. (6) However, these conditions are widely believed to be underdiagnosed, suggesting the true prevalence may be higher than current estimates indicate. (7)
Several epidemiologic patterns are well established:
Children and adolescents show the highest prevalence due to naturally increased joint laxity. (8)
Women are affected more frequently than men, with approximately a 2:1 ratio reported in many studies. (9,10)
Hypermobility tends to decrease with age as connective tissues stiffen.
Symptoms often begin early in life, yet the underlying condition may not be recognized until much later. As a result, many patients experience a prolonged diagnostic journey, often averaging a decade, before receiving an accurate explanation for their symptoms. (1)
3. What are the Symptoms of Joint Hypermobility Syndrome and Hypermobility Spectrum Disorders
Spinal Pain and Instability
Studies consistently show that the back (94%) and neck (20%) are among the most commonly reported symptomatic regions in hypermobile individuals. (9)
Over time, chronic joint laxity may contribute to premature degenerative change and conditions such as spondylolysis or spondylolisthesis, reflecting the inability of lax spinal ligaments to adequately restrain segmental motion. (11,12)
Hypermobility syndrome can also affect the upper cervical spine, where significant instability at the C0–C1 and C1–C2 levels may produce symptoms such as presyncope, dizziness, drop attacks, and cognitive “brain fog.” These patients often demonstrate high irritability to vertical posture or rapid neck movements. (13)
Peripheral Joint Pain and Injury
Hypermobile patients frequently present with recurrent peripheral complaints, including:
Chronic joint pain
Joint clicking or popping
Recurrent sprains or dislocations
Tendinopathy and soft-tissue injuries
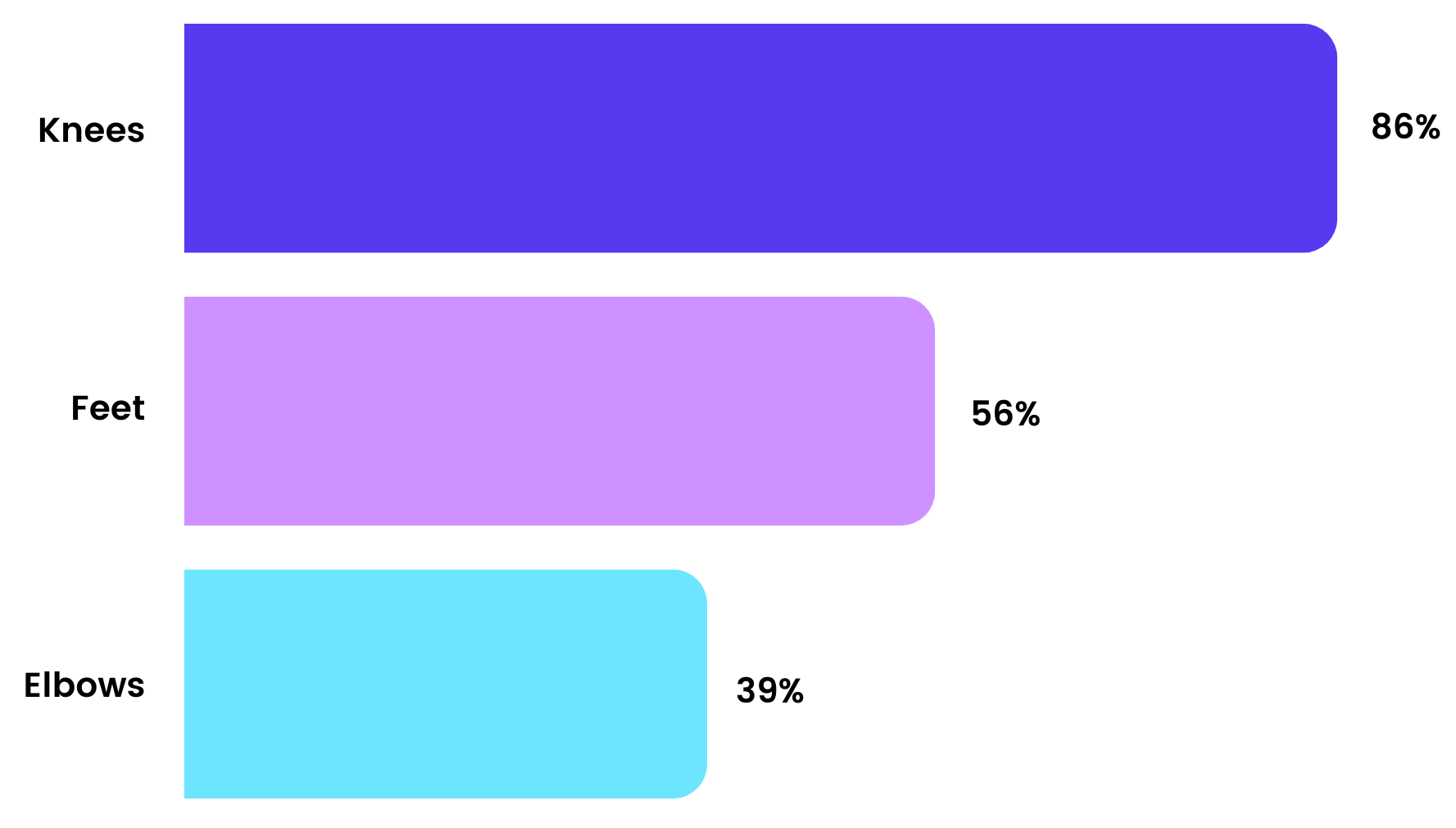
Symptoms commonly involve multiple regions of the body, including the knees (86%), feet (56%), and elbows (39%), reflecting the high mechanical demands placed on these joints during daily activity. (9)
In many cases, the pain is not simply intermittent soreness but a persistent and systemic experience, with patients frequently describing it as: (9)
Tiring and exhausting (93%)
Chronic and constant (67%)
Severe to very severe (66%)
In addition to ligamentous laxity, hypermobile individuals often exhibit impaired proprioception and neuromuscular control. (14) Clinically, this may present as:
Clumsiness
Poor motor control
Recurrent injury
Joint dislocations
Extra-Articular Manifestations
Hypermobility Spectrum disorders are increasingly recognized as a multisystem connective tissue condition with a wide range of associated features.
Headaches and migraines (11,15)
Peripheral entrapment neuropathies (16)
Dizziness (9,11)
Easy bruising and skin fragility (17-20)
Gastrointestinal symptoms such as abdominal pain or nausea (9,21-23)
Tachycardia (9)
Pelvic organ prolapse (9)
Anxiety and panic disorders (9,24,25)
Fatigue and sleep disorders* (11,16)
*Generalized fatigue is a hallmark feature, affecting the vast majority of individuals, and can significantly impair daily functioning and recovery. (9)
Because of this broad symptom profile, hypermobility-related conditions are frequently misdiagnosed as fibromyalgia or other chronic pain syndromes, delaying appropriate recognition and treatment. (9,26)
4. How to Diagnose Joint Hypermobility Syndrome (Beighton Score and Screening Tests)
Red Flags for Hypermobility in the Chiropractic Clinic
Chronic pain with normal imaging
Repeated sprains or joint injuries
Frequent treatment relapse
Difficulty tolerating high-velocity manipulation
Excessive spinal end-range motion on palpation
Questionairres
The Hakim and Grahame questionnaire can help identify hypermobility syndrome by asking patients if they:
Consider themselves “double-jointed.”
Could place palms flat on the floor without bending the knees
Could bend their thumb to the forearm
Performed contortionist movements as a child
Experienced recurrent joint dislocations
A positive response to two or more questions has demonstrated 85% sensitivity and 90% specificity for detecting hypermobility. (7,27)
Pro tip: ChiroUp subscribers can access hundreds of clinical forms, including a large selection of functional disability and screening surveys. Visit Practice Resources > Forms Library and search for your favorites, including the Hakim and Grahame Questionnaire.
Clinicians can also reference the 2017 International Consortium diagnostic criteria for hypermobile Ehlers-Danlos syndrome (hEDS), an easy-to-use clinical checklist outlining the three diagnostic domains when a more significant connective-tissue disorder is suspected. (28)
Assessments
Before applying formal scoring tools, clinicians should assess both the symptomatic joint and overall joint mobility, using range of motion testing and motion palpation to determine whether a tender segment is hypermobile or hypomobile.
What is the Beighton score?
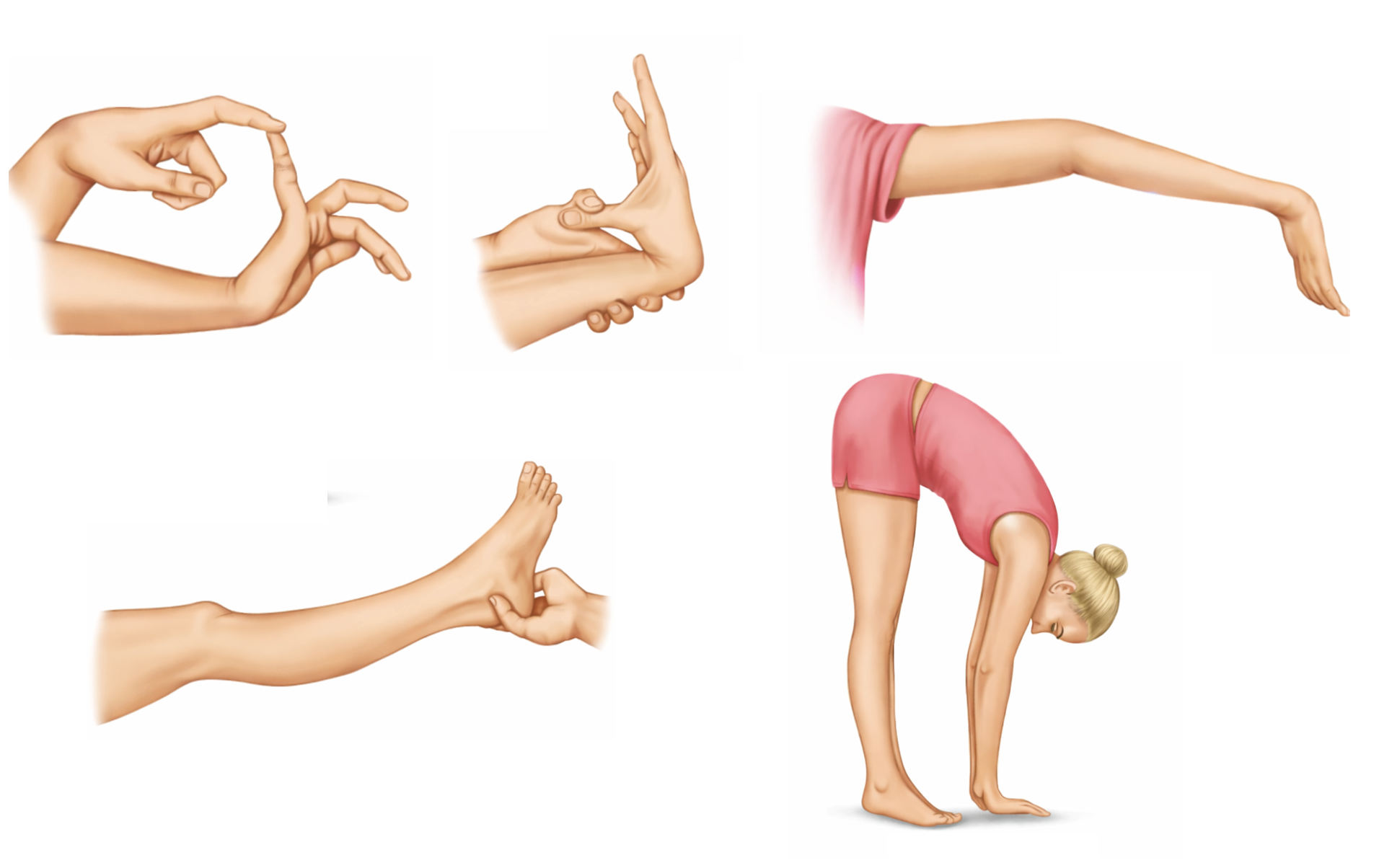
The Beighton score is the most widely used clinical tool for assessing generalized joint hypermobility. (29) It evaluates five joint movements:
Passive fifth finger extension ≥90°
Thumb to forearm apposition
Elbow hyperextension ≥10°
Knee hyperextension ≥10°
Forward trunk flexion with palms flat on the floor
Because the first four maneuvers are assessed bilaterally, one point is awarded for each side, while the trunk flexion test is scored once, producing a maximum score of nine points. A score of 4/9 or greater is commonly used as a diagnostic threshold for hypermobility.
ChiroUp subscribers can review a step-by-step video tutorial of the Beighton evaluation here.
Additionally, spinal segmental instability can be evaluated using a well-established cluster of clinical tests designed to assess excessive motion and impaired segmental control.

Apprehension Sign

Instability Catch Sign

Painful Catch Sign

Prone Instability Test
Pro tip: For a detailed overview of the assessment and management tools for lumbar instability, please refer to our prior blog on Lumbar Instability.
5. Treatment for Joint Hypermobility: Chiropractic and Rehabilitation Strategies
Traditional chiropractic care often focuses on restoring mobility to restricted spinal segments. In patients with generalized joint hypermobility, however, excessive motion may already exist within the joint complex, creating a clinical paradox: treatments designed to increase mobility may aggravate symptoms if underlying instability is not addressed.
Common Treatment Mistakes in Hypermobile Patients
Repeated manipulation of already unstable segments
Overstretching exercises that increase joint laxity
Rapid exercise progression leading to injury
Ignoring proprioceptive deficits
For this reason, the primary goal of treatment should be improving joint stability through active rehabilitation and neuromuscular control rather than passive mobilization alone.
Should hypermobile patients avoid spinal manipulation?
Spinal manipulation is not necessarily contraindicated in patients with generalized hypermobility. Clinical reports suggest that carefully selected manipulative treatments may still provide benefit when true segmental restriction is present and when manipulation is integrated into a broader, stability-focused care plan. (30) Several important considerations apply:
Target only clearly hypomobile segments, avoiding repeated treatment of already lax joints. (31)
Expect reduced tolerance to forceful interventions, as ligamentous laxity and altered pain processing may increase sensitivity to manual therapies. (30,32)
Consider modifying techniques, including reducing thrust force, amplitude, or frequency of care. (30)
Educate patients that post-treatment soreness may occur more frequently than in non-hypermobile individuals. (30,32)
In practice, manipulation should therefore be applied judiciously and strategically, while the overall treatment plan prioritizes strengthening, proprioceptive retraining, and strategies that enhance joint stability. (31)
6. Evidence-Based Exercises for Hypermobility Syndrome
The cornerstone of hypermobility management is strengthening and neuromuscular control to improve dynamic joint stability and compensate for ligamentous laxity. Evidence suggests that stabilization programs can reduce pain and improve postural stability in patients with hypermobility. (33)
Recommended activities to improve both muscular support and proprioception include:
Pilates or yoga
Tai Chi
Swimming
Spinal stabilization exercises
Resistance training
Specific resistance training prescriptions should be tailored to the patient’s primary sites of involvement. However, general considerations for a trunk stability program may include the following:

Bird Dog

Dead Bug

Side Bridge
Exercise should follow a graded progression, particularly in deconditioned individuals. Rapid increases in activity can potentially provoke injury due to insufficient joint stability. (34)
7. Practical ADL Advice for Hypermobile Patients
Lifestyle education plays an essential role in management. Patients should be instructed to:
Avoid end-range joint positions, particularly locking joints into hyperextension
Maintain slight flexion in the knees and elbows when standing to reduce ligament strain
Maintain neutral spinal posture during sitting and standing
Avoid prolonged slumped sitting or static positions
Optimize workstation ergonomics to minimize repetitive joint stress
Modify repetitive tasks and the pacing of physical activities to prevent overloading unstable joints
While active rehabilitation should remain the primary focus, clinicians may consider supportive options such as taping, splints, or compression garments to provide additional proprioceptive feedback and support for unstable joints.
Some patients may need to temporarily limit high-impact activities (i.e., contact sports) until adequate motor control is reestablished.
Finally, clinicians should set realistic expectations for recovery, as improvement in hypermobile patients is often slower than in non-hypermobile individuals due to the time required to restore joint proprioception and develop adequate muscular support. (35,36)
Pro tip: ChiroUp subscribers can download and share our newest Hypermobility Infographic by navigating to Practice Resources > Forms Library and searching “hypermobility.”

Conclusion
Joint hypermobility and hypermobility spectrum disorders are common but frequently overlooked causes of chronic musculoskeletal pain. Chiropractors play a key role in identifying these patients through screening tools such as the Beighton score and targeted clinical history. Effective care focuses on improving joint stability, proprioception, and neuromuscular control rather than increasing mobility alone.
Clinical Takeaways for Chiropractors
Hypermobility affects 10–30% of the population
Symptoms often include chronic pain, fatigue, and recurrent injury
The Beighton score is the most common screening test
Treatment should emphasize stability and proprioception, not additional mobility
Your patients deserve the most informed, evidence-based care, and you deserve tools that make it simple. ChiroUp puts hundreds of assessments and functional forms at your fingertips.
Sign up for free access now and start applying these resources in your practice immediately.
Quick FAQs
What is hypermobility spectrum disorder (HSD)?
Hypermobility spectrum disorder describes symptomatic joint hypermobility that does not meet diagnostic criteria for hypermobile Ehlers-Danlos syndrome.
How common is joint hypermobility?
Joint hypermobility traits occur in approximately 10–30% of the population, while symptomatic hypermobility spectrum disorders affect roughly 1–4%.
What are common symptoms of hypermobility?
Chronic spine or joint pain
Frequent sprains or dislocations
Fatigue
Poor proprioception
Dizziness or autonomic symptoms
What is the Beighton score?
The Beighton score is a nine-point clinical assessment used to evaluate generalized joint hypermobility. It measures five movements, including finger extension, thumb-to-forearm contact, elbow and knee hyperextension, and trunk flexion.
-
1. Palmer S, Bridgeman K, Di Pierro I, Jones R, Phillips C, Wilson M. The views of people with joint hypermobility syndrome on its impact, management and the use of patient‐reported outcome measures. A thematic analysis of open‐ended questionnaire responses. Musculoskeletal Care. 2019 Jun;17(2):183-93. Link
2. Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. A framework for the classification of joint hypermobility and related conditions. InAmerican Journal of Medical Genetics Part C: Seminars in Medical Genetics 2017 Mar (Vol. 175, No. 1, pp. 148-157). Link
3. Malfait F, Francomano C, Byers P, Belmont J, Berglund B, Black J, Bloom L, Bowen JM, Brady AF, Burrows NP, Castori M. The 2017 international classification of the Ehlers–Danlos syndromes. InAmerican Journal of Medical Genetics Part C: Seminars in Medical Genetics 2017 Mar (Vol. 175, No. 1, pp. 8-26). Link
4. Russek LN, Errico DM. Prevalence, injury rate and, symptom frequency in generalized joint laxity and joint hypermobility syndrome in a “healthy” college population. Clinical rheumatology. 2016 Apr;35(4):1029-39. Link
5. Hypermobility Syndromes Association (2022) Hypermobility syndromes association home. Accessed March 13, 2026 via Link
6. Kumar B, Lenert P. Joint hypermobility syndrome: recognizing a commonly overlooked cause of chronic pain. The American journal of medicine. 2017 Jun 1;130(6):640-7. Link
7. Carroll MB. Hypermobility spectrum disorders: A review. Rheumatology and immunology research. 2023 Jul 22;4(2):60-8. Link
8. Reuter PR, Fichthorn KR. Prevalence of generalized joint hypermobility, musculoskeletal injuries, and chronic musculoskeletal pain among American university students. PeerJ. 2019 Sep 11;7:e7625. Link
9. Clark NL, Johnson M, Rangan A, Kottam L, Swainston K. The biopsychosocial impact of hypermobility spectrum disorders in adults: a scoping review. Rheumatology International. 2023 Jun;43(6):985-1014. Link
10. Simmonds JV, Keer RJ. Hypermobility and the hypermobility syndrome. Manual therapy. 2007 Nov 1;12(4):298-309. Link
11. Hope L, Juul-Kristensen B, Løvaas H, Løvvik C, Maeland S. Subjective health complaints and illness perception amongst adults with Joint Hypermobility Syndrome/Ehlers–Danlos Syndrome-HypermobilityType–a cross-sectional study. Disability and rehabilitation. 2019 Jan 30;41(3):333-40. Link
12. Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers–Danlos syndrome (hypermobility type): it is a challenge. Journal of pain research. 2015 Aug 20:591-601. Link
13. Russek LN, Block NP, Byrne E, Chalela S, Chan C, Comerford M, Frost N, Hennessey S, McCarthy A, Nicholson LL, Parry J. Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: International expert consensus recommendations. Frontiers in medicine. 2023 Jan 18;9:1072764. Link
14. Akaras E, Deniz G, Eymir M, Sönmez M. The effects of joint hypermobility on strength, proprioception, and functional performance. Scientific Reports. 2025 Nov 18;15(1):40529. Link
15. Puledda F, Viganò A, Celletti C, Petolicchio B, Toscano M, Vicenzini E, Castori M, Laudani G, Valente D, Camerota F, Di Piero V. A study of migraine characteristics in joint hypermobility syndrome aka Ehlers–Danlos syndrome, hypermobility type. Neurological Sciences. 2015 Aug;36(8):1417-24. Link
16. Hakim A. Hypermobile ehlers-danlos syndrome. GeneReviews®[Internet]. 2024 Feb 22. Link
17. Mishra MB, Ryan P, Atkinson P, Taylor H, Bell J, Calver D, Fogelman L, Child A, Jackson G, Chambers JB, Grahame R. Extra-articular features of benign joint hypermobility syndrome. Rheumatology. 1996 Sep 1;35(9):861-6. Link
18. Folci M, Capsoni F. Arthralgias, fatigue, paresthesias and visceral pain: can joint hypermobility solve the puzzle? A case report. BMC musculoskeletal disorders. 2016 Feb 4;17(1):58. Link
19. Baeza-Velasco C, Van den Bossche T, Grossin D, Hamonet C. Difficulty eating and significant weight loss in joint hypermobility syndrome/Ehlers–Danlos syndrome, hypermobility type. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity. 2016 Jun;21(2):175-83. Link
20. Lee M, Strand M. Ehlers–Danlos syndrome in a young woman with anorexia nervosa and complex somatic symptoms. International Journal of Eating Disorders. 2018 Mar;51(3):281-4. Link
21. Zarate N, Farmer AD, Grahame R, Mohammed SD, Knowles CH, Scott SM, Aziz Q. Unexplained gastrointestinal symptoms and joint hypermobility: is connective tissue the missing link?. Neurogastroenterology & motility. 2010 Mar;22(3):252-e78. Link
22. Hope L, Juul-Kristensen B, Løvaas H, Løvvik C, Maeland S. Subjective health complaints and illness perception amongst adults with Joint Hypermobility Syndrome/Ehlers–Danlos
Syndrome-HypermobilityType–a cross-sectional study. Disability and rehabilitation. 2019 Jan
30;41(3):333-40. Link
23. Palmer S, Bridgeman K, Di Pierro I, Jones R, Phillips C, Wilson M. The views of people with joint hypermobility syndrome on its impact, management and the use of patient‐reported outcome measures. A thematic analysis of open‐ended questionnaire responses. Musculoskeletal Care. 2019 Jun;17(2):183-93. Link
24. Bulbena A, Gago J, Pailhez G, Sperry L, Fullana MA, Vilarroya O. Joint hypermobility syndrome is a risk factor trait for anxiety disorders: a 15-year follow-up cohort study. General Hospital Psychiatry. 2011 Jul 1;33(4):363-70. Link
25. Kumar B, Lenert P. Joint hypermobility syndrome: recognizing a commonly overlooked cause of chronic pain. The American journal of medicine. 2017 Jun 1;130(6):640-7. Link
26. Clark CJ, Khattab AD, Carr EC. Chronic widespread pain and neurophysiological symptoms in joint hypermobility syndrome (JHS). International Journal of Therapy and Rehabilitation. 2014 Feb;21(2):60-7. Link
27. Hakim AJ, Grahame R. A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain. International journal of clinical practice. 2003 Apr;57(3):163-6. Link
28. Malfait F, Francomano C, Byers P , Belmont J, Berglund B, Black J, Bloom L, Bowen JM, Brady AF, Burrows NP , Castori M. The 2017 international classification of the Ehlers–Danlos
syndromes. InAmerican Journal of Medical Genetics Part C: Seminars in Medical Genetics 2017
Mar (Vol. 175, No. 1, pp. 8-26). Link
29. Beighton PH, Solomon L, Soskolne CL. Articular mobility in an African population. Annals of the rheumatic diseases. 1973 Sep;32(5):413. Link
30. Boudreau PA, Steiman I, Mior S. Clinical management of benign joint hypermobility syndrome: a case series. The Journal of the Canadian Chiropractic Association. 2020 Apr;64(1):43. Link
31. Russek LN. Examination and treatment of a patient with hypermobility syndrome. Physical Therapy. 2000 Apr 1;80(4):386-98. Link
32. Grahame R. Joint hypermobility and genetic collagen disorders: are they related?. Archives of disease in childhood. 1999 Feb 1;80(2):188-91. Link
33. Toprak Celenay S, Ozer Kaya D. Effects of spinal stabilization exercises in women with benign joint hypermobility syndrome: a randomized controlled trial. Rheumatology international. 2017 Sep;37(9):1461-8. Link
34. Grahame R. Pain, distress and joint hyperlaxity. Joint Bone Spine. 2000 Jan 1;67(3):157-63. Link
35. Simmonds JV, Keer RJ. Hypermobility and the hypermobility syndrome. Manual therapy. 2007 Nov 1;12(4):298-309. Link