
Chiropractic E/M Coding Guide Part 2: Medically Appropriate History and Examination
In this second part of our E/M coding series, we focus on one of the most misunderstood areas in chiropractic documentation: medically appropriate history and examination. While E/M coding now centers on time or medical decision-making, proper chiropractic SOAP note documentation, patient history, and clinical examination remain essential for compliance, audit protection, and accurate chiropractic billing.
Evaluation and management (E/M) coding changed dramatically in 2021 when the three key components of history, exam, and medical decision making were replaced and modified. Instead, codes were to be selected by either time or medical decision-making. The history and the exam took a back seat, at least in terms of code selection. However, they are still an essential part of the documentation.
History and Examination in Chiropractic E/M Coding
History and examination are not factors that affect the choice of an E/M code. The guidelines tell us that they should be “medically appropriate”, and the treating physician can determine the nature and extent of the history and examination. Information for the history can be gathered by the care team, a paper questionnaire, or an electronic health record portal, but it must be reviewed by the reporting physician. In a record, that means that there must be some acknowledgment or statement by the provider that the information was considered.
One way to determine if you have documented sufficient history and examination is to consider what a panel of your peers would feel is “medically appropriate” for a patient in similar circumstances. Prior to 2021, these elements were laid out very specifically, and, as such, it might be useful to consider the old standard as a minimum amount of history and exam required to meet a “medically appropriate” threshold.
New Chiropractic Patients: History and Examination Requirements
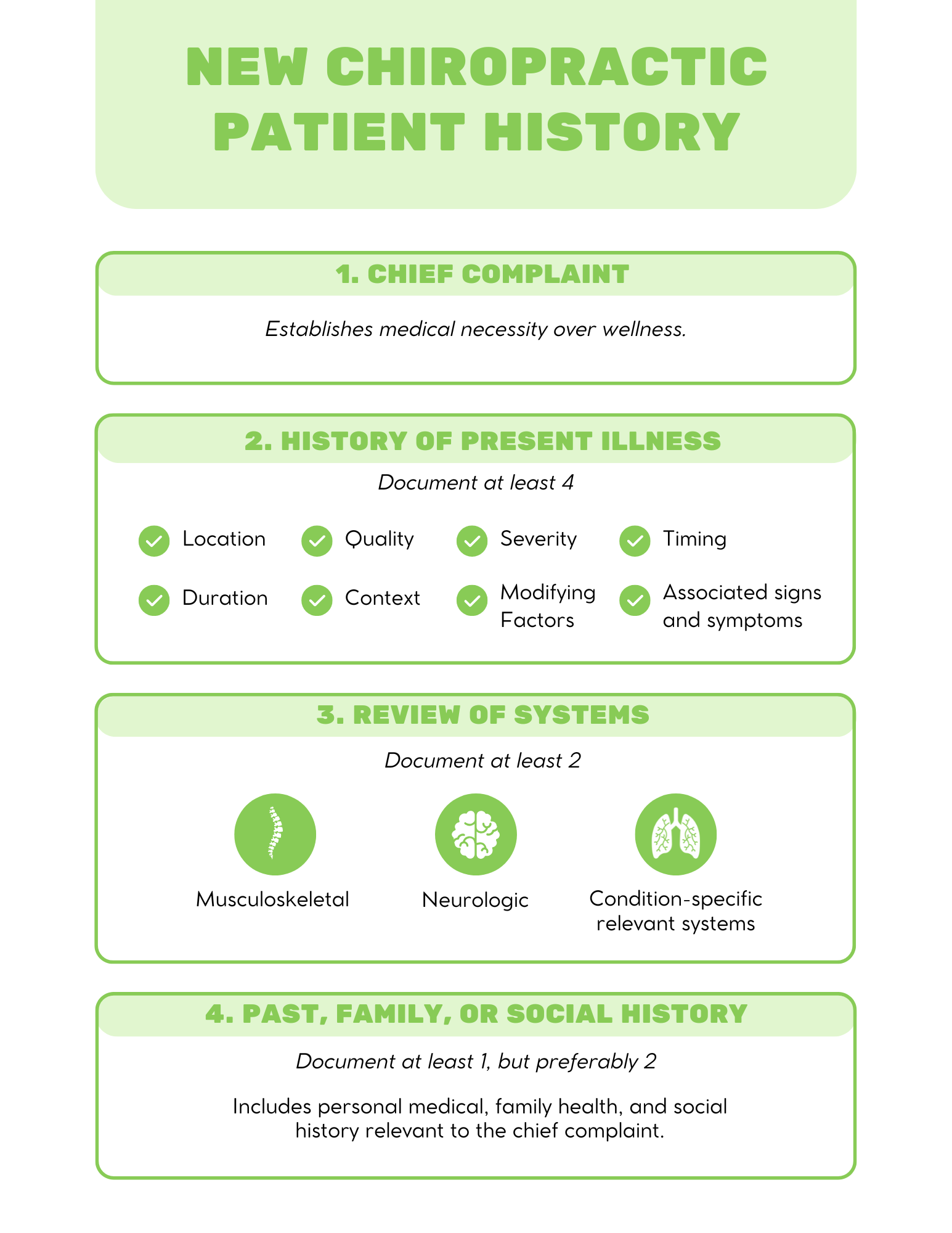
For new patients, consider the following minimum elements (as borrowed from the 1995 E/M guidelines for a 99203) as a standard for a medically appropriate history for a typical chiropractic patient:
1. Chief complaint (without one, the service would be a wellness visit, which often is not covered by third-party payers)
2. History of present illness (document at least 4, for each complaint):
Location
Quality
Severity
Timing
Duration
Context
Modifying factors
Associated signs and symptoms
3. Review of systems (document at least 2):
Musculoskeletal (could easily always include this one)
Neurologic (easily included in a typical chiropractic setting as well)
Condition-specific relevant systems (such as skin, heart, lungs, etc.)
4. Past, family, and/or social history (at least 1, but preferably 2)
The history information comes from the patient, whereas the exam information comes from the clinician. For a “medically appropriate” examination, consider that the old guidelines required an evaluation of at least two organ systems to reach a level 3 E/M code. Therefore, the minimum threshold for a typical chiropractic patient might be at least some documentation around a:
Musculoskeletal exam
Neurological exam
Other relevant body systems (vitals, skin, etc.)
Please note that none of these elements are specifically required per the 2021 updates to the guidelines; rather, they are offered here as suggestions for establishing a minimum standard in your office that would be easy to defend to a peer reviewer as “medically appropriate”.
Established Chiropractic Patients: Documentation Differences
Based on the 1995 rules for established patients, the requirements are not so stiff. You would still need a chief complaint and updates to the elements of the history of present illness documented at the new patient exam, but the other history elements do not need to be repeated, as they are likely unchanged. The exam can include just one organ system, most likely the musculoskeletal, if the other systems examined previously were determined not to be relevant. But more systems can be included if they have positive findings at the previous exam.
How History and Exam Impact Chiropractic E/M Code Selection
Per the 2021 update to E/M codes, once the history and exam are documented, providers select the code based on time or medical decision-making. The documentation should be roughly equivalent in either case in terms of the standard of care, but each method has advantages and disadvantages.
FAQs
-
Medically appropriate means the history and examination should be sufficient for the patient’s condition and clinical presentation, as determined by the provider’s professional judgment.
-
Yes. While they no longer determine the code level, history and exam remain essential for supporting medical necessity and proper clinical documentation.
-
There is no strict requirement under current guidelines, but documentation should typically include chief complaint, relevant history of present illness, and appropriate review of systems based on the patient’s condition.
-
There is no required number, but documentation should reflect systems relevant to the patient’s condition, most commonly musculoskeletal and neurological findings.
-
They do not directly determine the E/M code, but incomplete documentation can still lead to denied claims or audit risk if medical necessity is not supported.
Conclusion
Accurately documenting medically appropriate history and examination is key to proper E/M coding in chiropractic practice. Chiropractors should ensure documentation reflects the patient’s clinical presentation, supports medical necessity, and aligns with current chiropractic billing and E/M coding guidelines.
Want to eliminate E/M coding guesswork? ChiroUp’s EHR helps guide documentation and coding based on clinical inputs, helping you stay compliant and efficient. See how it works in a quick demo.
This is Part 2 of a 4-part E/M Coding Mastery Series. Stay tuned for the following parts to be released over the next few months:
Part 1: Chiropractic E/M Coding Guide Part 1: New vs. Established Patients (99201–99215 Explained)
Part 2: Medically Appropriate History and Examination
Part 3: Coding Using Time
Part 4: Coding Based on Medical Decision Making