
Treating Achilles Tendinopathy in Non-Athletes
Reading time: 5 minutes
The Achilles tendon is the largest and strongest tendon in the human body but is simultaneously a weak link in the locomotion chain. The tendons' structural prowess is relentlessly confronted by functional demands that can be up to 12 ½ times body weight while running. (1) The Achilles tendon may be acutely strained or ruptured due to an excessive stretch or eccentric force.
There are three important features of non-insertional Achilles tendinopathy every evidence-based chiropractor must know.
How can you properly identify insertional vs non-insertional tendinopathy?
Initially, should you rest or rehabilitate these patients?
What rehabilitation exercises will speed up your patient’s recovery and improve your clinical results?
Today’s blog will focus on one type of Achilles tendinopathy often seen in chiropractic offices, non-insertional Achilles tendinopathy. This disorder is more common in our non-athletes. It has recognizable symptoms and signs and is treated very differently than its cousin—insertional Achilles tendinopathy. For a full review of insertional versus non-insertional Achilles tendinopathy, check out the condition reference in ChiroUp.
1. Identify Non-Insertional Achilles Tendinitis
Location. Location. Location.
Non-insertional Achilles tendinitis most commonly involves the vulnerable "watershed area," 2-6 cm proximal to the calcaneal insertion. (2) This tendon region has a smaller cross-sectional area, is relatively hypovascular, and is subject to a repetitive “wringing” motion during supination/ pronation. This susceptible mid-section is the most common site for degeneration and rupture. (1) Patients will often present with thickening of the Achilles tendon on the affected side with associated inflammation and pain.
2. Should I Rest Achilles Tendinopathy?
No. Most people consider Achilles tendinopathy an athlete’s injury, which would be an inappropriate assumption for non-insertional tendinopathy. In research by Kvist, 66% of patients with Achilles tendinopathy suffer from the non-insertional type. (3) Patients with non-insertional Achilles tendinopathy injuries tend to be older, less active, and overweight. (4) The last thing we should do with this population is to become less active. These patients will benefit from addressing key modifiable contributors to their injury listed below. (1)
Intrinsic Factors: foot hyperpronation, pes planus or cavus, gastrocnemius/posterior tibialis/soleus inflexibility or weakness, limited ankle dorsiflexion, and limited subtalar motion.
Systemic risk factors: diabetes, hypertension, inflammatory arthropathy, gout, and the use of corticosteroids or fluoroquinolone antibiotics.
Obesity: Obese patients carry a 4-6 fold higher risk of developing Achilles tendinopathy.
3. What Are The Best Exercises For Achilles Tendinopathy?
The good thing about non-insertional tendinitis is that there are a couple of research-backed exercises patients can do at home or within your office. These exercises will address the two most common weaknesses associated with Achilles tendinopathy: the soleus and the posterior tibialis.
The Soleus
Why Strengthen the Soleus?
Researchers from the United Kingdom found that patients who were overly flexible in the foot and had weak calves developed Achilles injuries at a much higher rate. These authors identified the soleus as a muscle weakness that likely predisposed the Achilles injury. Walking or running exposes the soleus to more stress than the gastrocnemius. Weakness or injury to the soleues results transfer of excess load to the Achilles tendon. (5) Strength deficits to the soleus are catastrophic to the gastrocnemius muscle and Achilles tendon. So traditional Achilles tendon rehab should be modified to include a bent knee exercise that targets this muscle.
How to Strengthen the Soleus
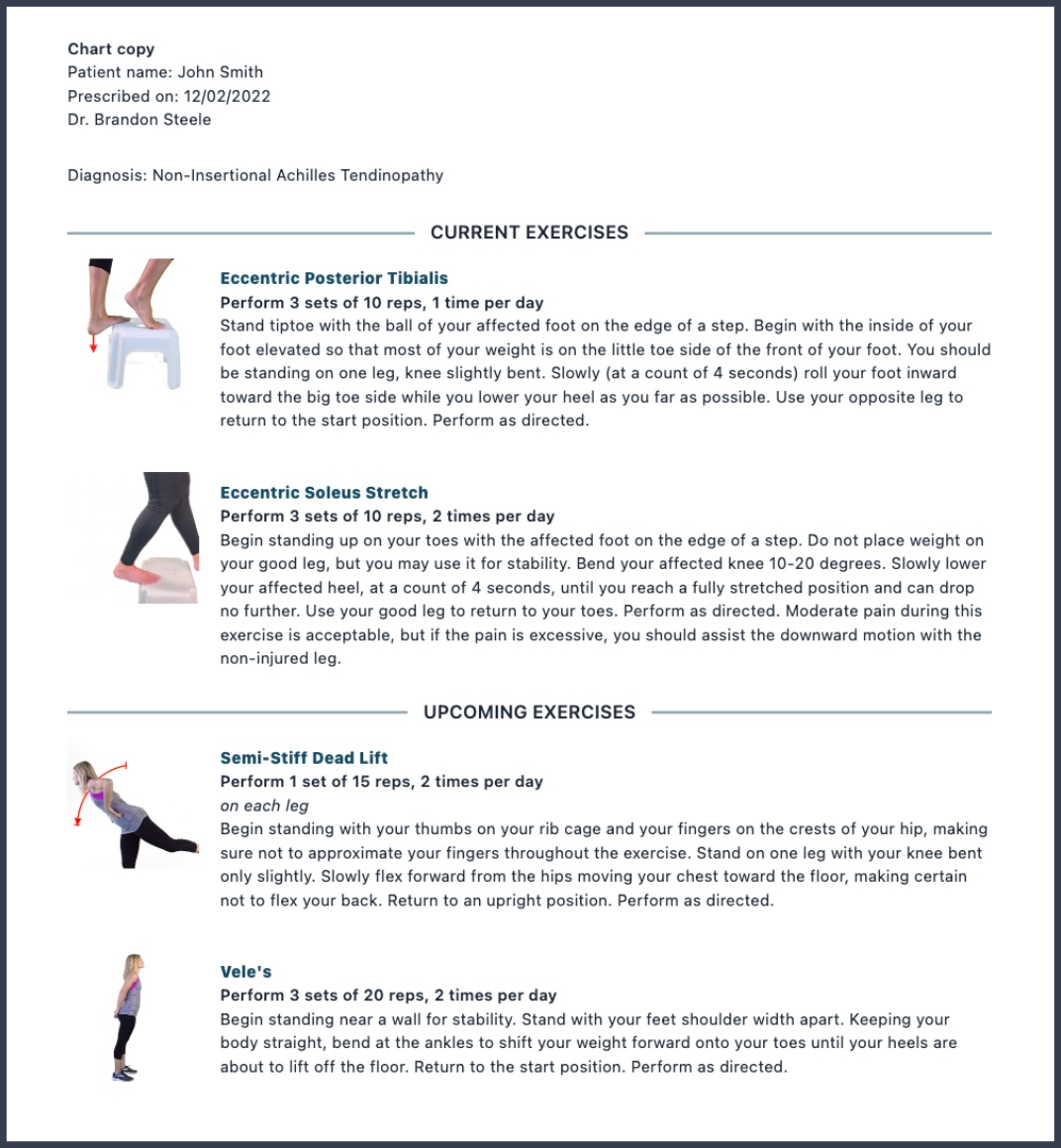
Begin standing up on your toes with the affected foot on the edge of a step. Do not place weight on your good leg, but you may use it for stability. Bend your affected knee 10-20 degrees and maintain knee bend through the exercise. Slowly lower your affected heel, at a count of 4 seconds, until you reach a fully stretched position and can drop no further. Use your good leg to return to your toes. Perform as directed. Moderate pain during this exercise is acceptable, but if the pain is excessive, you should assist the downward motion with the non-injured leg.

The Posterior Tibialis
Why Strengthen the Posterior Tibialis?
A patient suffering from a non-insertional Achilles injury also responds to strengthening the posterior tibialis. Weakness within the posterior tibialis results in a lack of foot external rotation and supination. Inefficient supination will place excessive strain on the Achilles tendon during the push-off phase of gait.
How to Strengthen the Posterior Tibialis
Stand tiptoe with the ball of your affected foot on the edge of a step. Begin with the inside of your foot elevated so that most of your weight is on the little toe side of the front of your foot. You should be standing on one leg, knee slightly bent. Slowly (at a count of 4 seconds) roll your foot inward toward the big toe side while you lower your heel as far as possible. Use your opposite leg to return to the start position. Perform as directed.

Download the customized condition report for non-insertional Achilles tendinopathy here:
Assessment and treatment of extremity disorders are the Achilles' heel of many good evidence-based providers. Don't worry; puns are acceptable if used in moderation! 😊
If you have any questions about the differential diagnosis of the most common foot disorders, check out ChiroUp for our extensive list of the most common extremity diagnoses you will see in chiropractic practice. You can also check out our latest webinar on the three most common foot disorders below.
Solving Plantar Foot Pain Webinar
with Dr. Brandon Steele
-
T Bertelsman and B Steele. Achilles Tendinopathy. www.ChiroUp.com Accessed 11.28.22 https://app.chiroup.com/clinical-skills/conditions/3884470
Wren TA, Lindsey DP, Beaupré GS, Carter DR. Effects of creep and cyclic loading on the mechanical properties and failure of human Achilles tendons. Annals of biomedical engineering. 2003 Jun 1;31(6):710-7
Kvist M. Achilles tendon injuries in athletes. Annales Chirurgiae et Gynaecologiae. 1991;80(2):188–201.
Irwin T. A. Current concepts review: insertional Achilles tendinopathy. Foot and Ankle International. 2010;31(10):933–939. doi: 10.3113/fai.2010.0933.
O'Neill S, Barry S, Watson P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: the role of soleus. Physical Therapy in Sport. 2019 May 1;37:69-76.