
3 Essential Skills for Resolving Cubital Tunnel Syndrome
Reading time: 3 minutes
As an evidence-based chiropractor, you see enough cases of carpal tunnel syndrome to recognize that it’s the most pervasive peripheral nerve entrapment in the upper extremity, but did you know that cubital tunnel syndrome is the second most common? (1,18,20)
A September 2022 article in Orthopedic Reviews reminded us how frequently this problem presents.
“It is estimated that up to 5.9% of the general population have had symptoms of cubital tunnel syndrome [which], if left untreated, can significantly alter an individual's quality of life.” (23)
This week’s updated blog & video will demonstrate three essential tools to solve this frequently overlooked problem. You’ll learn the top assessment, treatment, and ulnar nerve floss exercise for cubital tunnel syndrome in less than three minutes!
1. What Is Cubital Tunnel Syndrome?
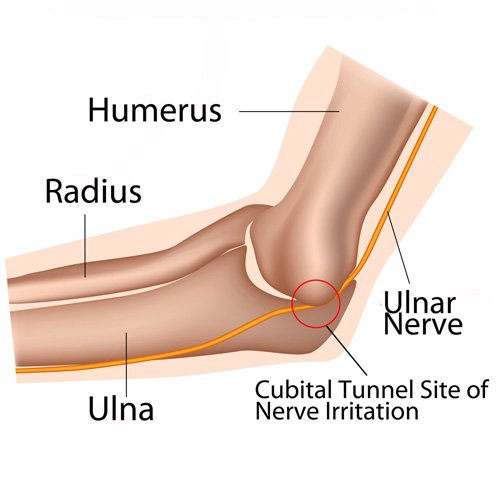
Short answer: Irritation of the ulnar nerve at the elbow.
Deeper dive: Elbow flexion requires the ulnar nerve to both stretch and slide through the cubital tunnel. As the elbow flexes, the distance between the medial epicondyle and olecranon increases, thereby stretching the ulnar nerve. Flexion also tensions the fascia resulting in ovoid deformation and reduced cubital tunnel volume. Sustained traction or compression may exceed the nerve's resiliency, leading to irritation and cubital tunnel syndrome symptoms (2).
2. What Are Cubital Tunnel Syndrome Symptoms?
Short answer: Pain or paresthesia in the 4th and 5th digits.
Deeper dive:
Patients with cubital tunnel often complain of symptoms extending distally from the medial epicondyle to the 4th and 5th digits.
Cubital tunnel symptoms may vary from vague hypersensitivity to pain.
Since motor fibers are located deep to sensory fibers, sensory irritation precedes motor deficits.
Like many other neuropathies, nocturnal symptoms are common.
Cubital tunnel syndrome presents 50% more frequently on the left side, regardless of handedness. (13)
3. Who Gets Cubital Tunnel Syndrome?
Short answer: Workers and athletes who repetitively flex or compress their elbow.
Deeper dive: Symptoms of cubital tunnel syndrome are commonly seen in baseball, tennis, and racquetball players. Workers who maintain sustained elbow flexion, such as holding a tool or telephone, or those who press the ulnar nerve against a hard surface, like a desk, are at increased risk. Cubital tunnel syndrome has more recently been coined cell phone elbow.
Did You Know?
Women’s elbows have a thicker fat pad on the medial aspect providing greater protection; men experience cubital tunnel syndrome complaints 3-8 times more often than women. (4)
4. What is the Best Cubital Tunnel Syndrome Test?
Short answer: The ulnar nerve tension test is the most useful diagnostic test for cubital tunnel syndrome. (6,7,8)
Deeper dive: The ulnar nerve tension test entails maintaining shoulder abduction while flexing the elbow past 90 degrees, supinating the forearm, and extending the wrist with thumb/ index opposition. A positive test results in the reproduction of the chief complaint within 60 seconds.


5. What Is the Best Cubital Tunnel Syndrome Treatment?
Short answer: Chiropractic manual therapy.
Deeper dive: Management of ulnar nerve compression includes activity modification, nerve mobilization techniques, myofascial release techniques, manipulation, splinting, and patient education. (11,20,23)
The cubital tunnel release, aka ulnar nerve release, is particularly beneficial for treating cubital tunnel syndrome. Subscribers can review this ulnar nerve release tutorial here.

6. What Is Ulnar Nerve Flossing for Cubital Tunnel Syndrome?
Short answer: Ulnar nerve flossing or ulnar nerve glide maneuvers are cornerstones of conservative cubital tunnel syndrome treatment.
Deeper dive: Flossing the ulnar nerve with an ulnar nerve glide or ulnar nerve floss has shown remarkable benefits for cubital tunnel patients. (22) Subscribers can review this ulnar nerve floss tutorial here.

Want to learn more about neurodynamic tests and treatments? Check out this prior blog detailing 3 Simple Nerve Flossing Exercises To Help Resolve Arm Pain.
7. What Are the Best Cubital Tunnel Syndrome Exercises?
Short answer: An ulnar nerve floss exercise.
Deeper dive: In addition to stretching the wrist flexors, cubital tunnel syndrome exercises should include an ulnar nerve self-floss.
Ulnar Nerve Floss
Hold your arm in front of you with your elbow, wrist, and fingers straight as though you are getting ready to shake hands. Touch the tips of your thumb and first finger together to make a ring. Slowly flex your elbow until your hand reaches your face. The ring position should be maintained, and your forefinger should be just beneath your eye socket. Slowly raise your elbow to flip the ring up into a monocle around your eye. Lower your arm back to the starting position and repeat ten repetitions three times per day or as directed.

To complement management and exercises for cubital tunnel syndrome, patients should consider the following home advice:
Limit prolonged flexion and direct pressure on the elbow.
Avoid sleeping with fully flexed elbows. A night-time cubital tunnel syndrome splint or cubital tunnel syndrome brace that limits flexion may be helpful. (30-45 degrees of flexion is thought to be the optimal position to decrease intraneural pressure). (9)
Consider a protective pad to limit repetitive daytime trauma from work or sports.
Want to automate your patient education and home exercise prescription? Did you know you can create a lay condition report, including video demonstrations of the most appropriate exercises, for any of the top 100+ chiropractic diagnoses in 4 clicks? Watch this video to see how.
-
1. Nicholas, J.A. The Upper Extremity in Sports Medicine, CV Mosby, 1990 p.343.
2. Wilgis EF, Murphy RD. The significance of longitudinal excursion in peripheral nerves. Hand clinics. 1986 Nov;2(4):761-6. Link
3. Charness ME. Unique upper extremity disorders of musicians. Occupational disorders of the upper extremity. New York: Churchill Livingstone. 1992 Jul:227-52.
4.Contreras MG, Warner MA, Charboneau WJ, Cahill DR. Anatomy of the ulnar nerve at the elbow: potential relationship of acute ulnar neuropathy to gender differences. Clinical Anatomy: The Official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists. 1998;11(6):372-8. Link
5. Sarwark JF. Essentials of musculoskeletal care. American Academy of Orthopedic Surgeons.
6. Buehler MJ, Thayer DT. The elbow flexion test. A clinical test for the cubital tunnel syndrome. Clinical orthopaedics and related research. 1988 Aug(233):213-6. Link
7. Rayan GM, Jensen C, Duke J. Elbow flexion test in the normal population. The Journal of hand surgery. 1992 Jan 1;17(1):86-9. Link
8. Ochi K, Horiuchi Y, Tanabe A, Morita K, Takeda K, Ninomiya K. Comparison of shoulder internal rotation test with the elbow flexion test in the diagnosis of cubital tunnel syndrome. The Journal of hand surgery. 2011 May 1;36(5):782-7. Link
9. Yamaguchi K, Sweet FA, Bindra R, Gelberman RH. The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. Journal of shoulder and elbow surgery. 1999 Jan 1;8(1):17-21. Link
10. Rayegani SM, Raeissadat SA, Kargozar E, Rahimi-Dehgolan S, Loni E. Diagnostic value of ultrasonography versus electrodiagnosis in ulnar neuropathy. Medical Devices (Auckland, NZ). 2019;12:81. Link
11. Kooner S, Cinats D, Kwong C, Matthewson GD, Dhaliwal G. Conservative treatment of cubital tunnel syndrome: A systematic review. Orthopedic Reviews. 2019 Jun 12;11(2). Link
12. Gündüz A, Candan F, Asan F, Uslu F, Uzun N, Karaali-Savrun F. Ulnar Neuropathy at Elbow in Patients With Type 2 Diabetes Mellitus. Journal of clinical neurophysiology: official publication of the American Electroencephalographic Society. 2019 Aug. Link
13. Ashworth NL, Huang C, Chan KM. Laterality and risk factors for ulnar neuropathy at the elbow. Muscle & Nerve. 2019 Oct 10. Link
14. Martínez-Aparicio C, Jääskeläinen SK, Puksa L, Reche-Lorite F, Torné-Poyatos P, Paniagua JS, Falck B. Constitutional risk factors for focal neuropathies in patients referred for EMG. European journal of neurology. 2019 Nov. Link
15. Lee SK, Hwang SY, Choy WS. Validity of computed tomographic measurements and morphological comparison of cubital tunnel in idiopathic cubital tunnel syndrome. BMC Musculoskeletal Disorders. 2020 Dec 1;21(1):76. Link
16. Rydberg M, Zimmerman M, Gottsäter A, Nilsson PM, Melander O, Dahlin LB. Diabetes mellitus as a risk factor for compression neuropathy: a longitudinal cohort study from southern Sweden. BMJ Open Diabetes Research and Care. 2020 Apr 1;8(1):e001298. Link
17. Lee SK, Hwang SY, Kim SG, Choy WS. Analysis of the Anatomical Factors Associated with Cubital Tunnel Syndrome. Orthopaedics & Traumatology: Surgery & Research. 2020 Apr 30. Link
18. Cutts S. Cubital tunnel syndrome. Postgraduate medical journal. 2007 Jan 1;83(975):28-31. Link
19. An TW, Evanoff BA, Boyer MI, Osei DA. The prevalence of cubital tunnel syndrome: a cross-sectional study in a US metropolitan cohort. The Journal of bone and joint surgery. American volume. 2017 Mar 1;99(5):408. Link
20. Chauhan M, Anand P, Das JM. Cubital Tunnel Syndrome. StatPearls [Internet]. 2020 Mar 24.Link
21. Kooner S, Cinats D, Kwong C, Matthewson G, Dhaliwal G. Conservative treatment of cubital tunnel syndrome: A systematic review. Orthopedic reviews. 2019 May 23;11(2). Link
22. Svernlöv B, Larsson M, Rehn K, Adolfsson L. Conservative treatment of the cubital tunnel syndrome. Journal of Hand Surgery (European Volume). 2009 Apr;34(2):201-7. Link
23. Anderson D, Woods B, Abubakar T, Koontz C, Li N, Hasoon J, Viswanath O, Kaye AD, Urits I. A Comprehensive Review of Cubital Tunnel Syndrome. Orthopedic Reviews. 2022 Sep 15;14(3). Link