
Performing the Modified Thomas Test (Part I)
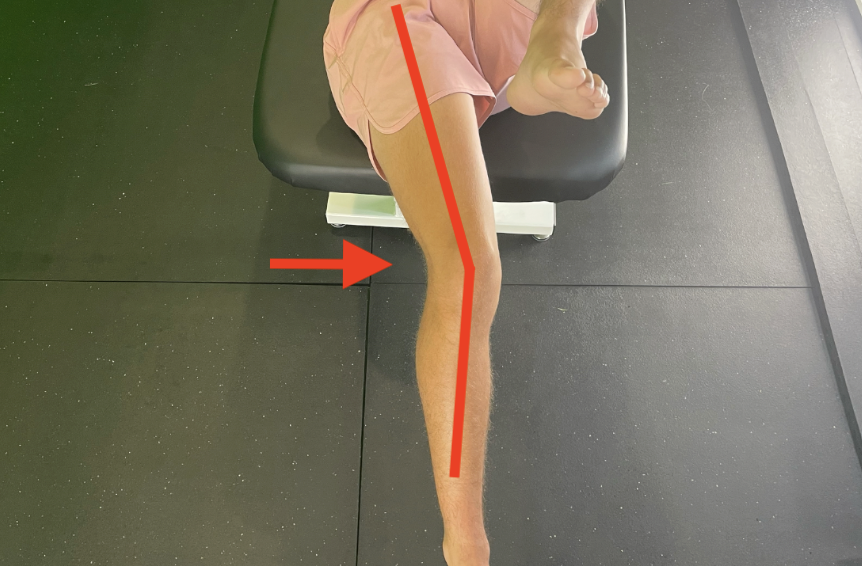
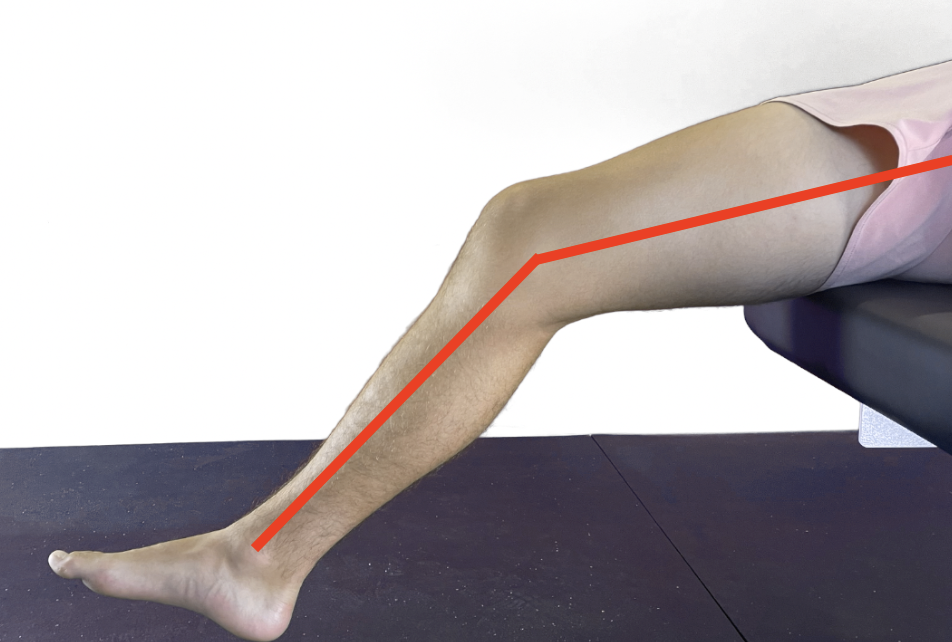
The supine patient performs a single knee-to-chest maneuver. The clinician observes the opposite thigh to determine whether it remains flat on the table or rises. Patients with excessive hip flexor tightness will flex or lift their straightened leg. (1)


The Modified Thomas test may become provocative for pain due to these orthopedic conditions during this test.
1. Low Back Pain
Excessive lumbar lordosis during the test suggests hip flexor tightness resulting in lumbar spine compensation.


2. Gluteal Tendinopathy and ITB Syndrome
Abduction and external rotation of the affected leg suggests hypertonicity with the TFL and external rotators of the hip.


3. Knee Osteoarthritis
Adduction of the hip suggests tightness in the hip adductors. Adductor hypertonicity is common in patients with knee OA as a protective mechanism.

4. Patellofemoral Pain Syndrome
Excessive knee extension demonstrates adaptively shortened quadriceps due to postural or repetitive load.

Positive (+)
Hip flexor hypertonicity may be due to several factors: including sitting for long periods, poor posture, or overuse injuries. Your treatment success depends on identifying the cause of hip flexor hypertonicity and not just treating the hypertonic muscles.
How to Stretch Tight Hip Flexors
Perform contract-relax stretching of the hip flexors and quadriceps from the test position. This approach offers several advantages for evidence-based chiropractors:
Time-saving: Utilizing the test position can optimize efficiency by minimizing the need to switch the patient's position repeatedly during treatment.
Rapid assessment and treatment: The practitioner can swiftly assess, treat, and re-assess hypertonic muscles in seconds, ensuring a prompt and targeted intervention.
Visible progress: Patients will experience tangible and immediate results by implementing straightforward muscle stretching techniques, enhancing their perception of the treatment's effectiveness.
For the complete list of treatments, including soft tissue manipulation, instrument, assisted manipulation, nerve, mobilization, and flossing, manipulation, and mobilization, check out the treatment technique section within ChiroUp.
Do Hip Flexors Affect Running?
Tight hip flexors can have many adverse effects on running, including:
Reduced stride length: When hip flexors are tight, they limit the range of motion, thereby shortening stride length while running. Runners with tight hip flexors are slower and less efficient.
Increased risk of injury: Tight hip flexors can stress other muscles and joints, increasing the risk of injuries such as runner's knee, IT band syndrome, and lower back pain.
Poor running form: Tight hip flexors can force you to overstride or to run with a forward lean, which can also increase your risk of injury commonly associated with back and knee pain.
Pain: Tight hip flexors can be painful, especially during the beginning of running or long-distance runs.
Don’t Forget to Re-Test After Treatment
Performing orthopedic tests is significant during the initial visit. But remember to recheck for your objective findings and show your patient's progress throughout the treatment plan. Continually reminding patients where they started compared to where they are will help them notice your treatment's effectiveness and improve compliance with their at-home rehabilitation exercises.
Want more? Check out Part II of this blog for using the Modified Thomas Test in a youth soccer player with LBP.
Speaking about patient compliance, we understand that it’s easier said than done. That’s where we come in. At ChiroUp, we provide the essential resources to effectively engage your patients and encourage them to become active participants in their recovery journey. Start your 14-day FREE trial with us and witness the positive impact on patient compliance.
-
Vigotsky AD, Lehman GJ, Beardsley C, Contreras B, Chung B, Feser EH. The modified Thomas test is not a valid measure of hip extension unless pelvic tilt is controlled. Peer J. 2016 Aug 11;4:e2325.