
Differentiating Plantar Fasciitis from the Imposters
Reading time: 5 minutes
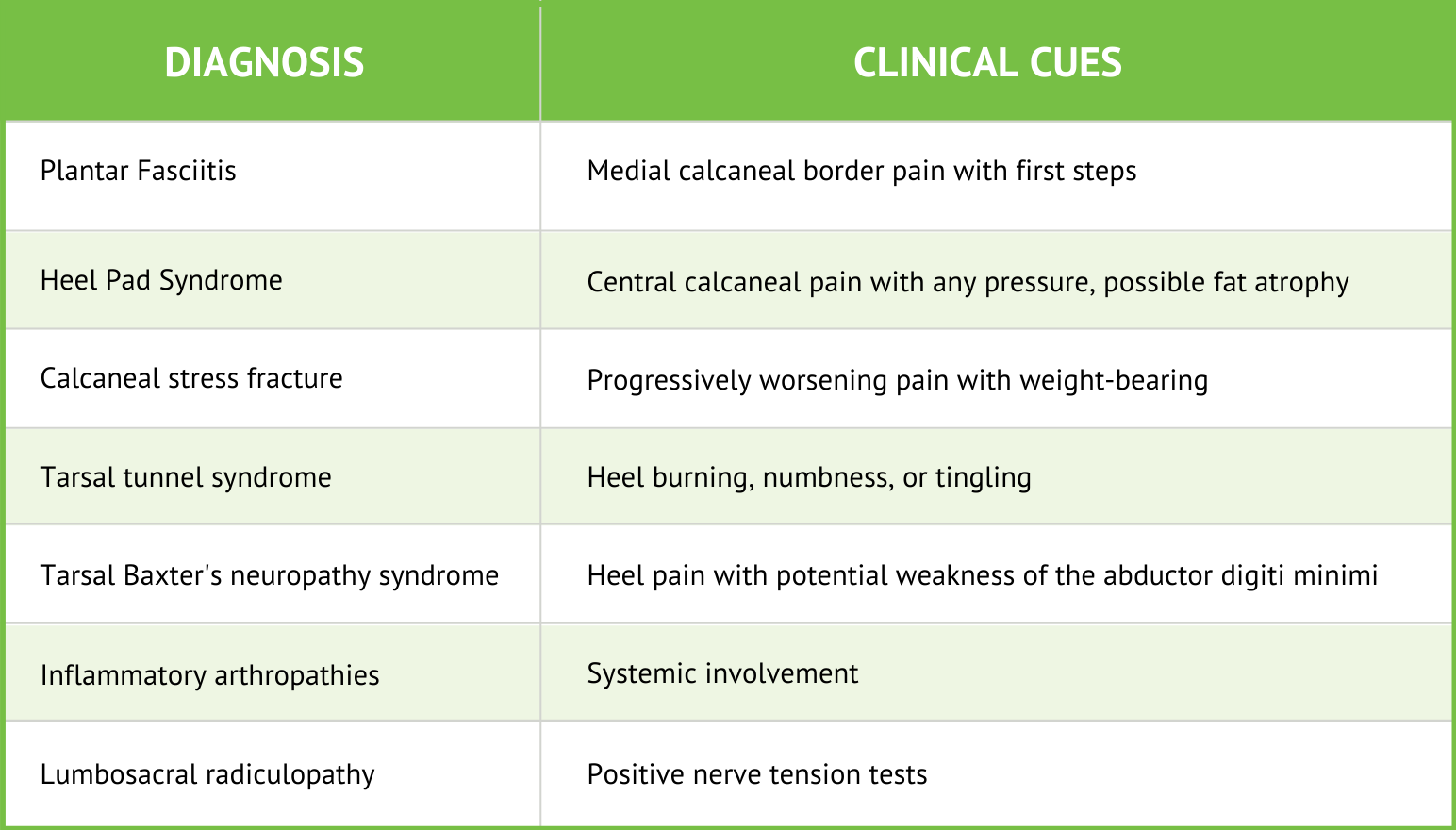
If a patient presents with plantar heel pain that surges when they step out of bed in the morning or start to walk, most evidence-based chiropractors think plantar fasciitis. But what if that’s not the diagnosis. There are several frequently overlooked possibilities in the differential diagnosis.
Watch this quick and valuable tutorial: Differential diagnosis of plantar heel pain.
Diving Into #2 🤔
Following plantar fasciitis, heel pad syndrome is the second most common cause of plantar heel pain, claiming approximately 15% of all presentations. (3,4) Up to one in ten people will suffer from heel pad syndrome at some point in their lifetime. (5)
Your ChiroUp team recently took a deep dive into Heel Pad Syndrome. With the help of a few experts like Tom Michaud, our advisory board has authored and released ChiroUp protocol #104- Heel Pad Syndrome. What did we learn? - A lot. Here’s our 2-minute, Top 10 Summary:
1. Anatomy
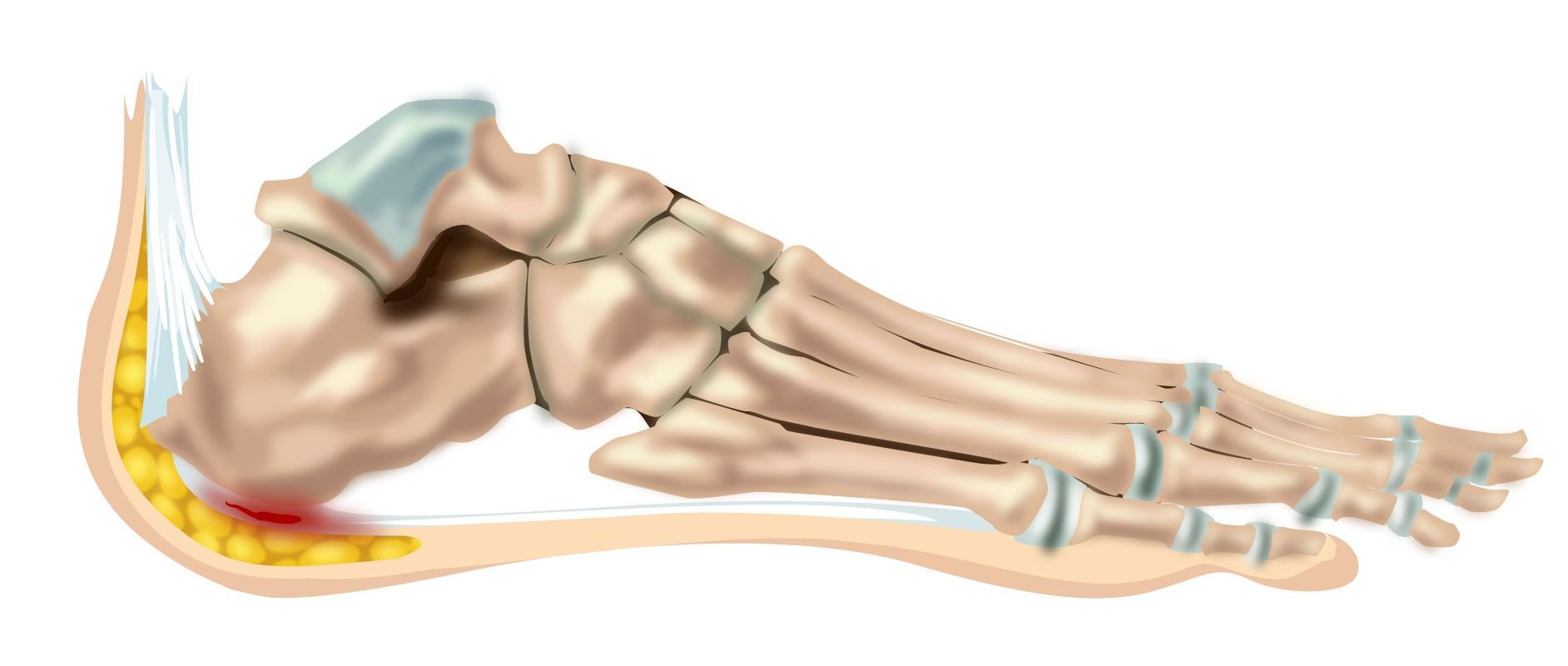
The heel fat pad is a specialized shock absorber that overlies the inferior and posterior calcaneus to impart cushioning and help dampen ground reaction forces. (7-10) The heel pad is composed of closely packed honeycombed fat globules held together by a collagenous septum. (6,11,12)
2. Etiology
Time and stress promote atrophy of the fat cells and degeneration of the fibrous septae. This leads to decreased elasticity and shock absorption, resulting in increased calcaneal pressure. (18-24) While atrophy and degeneration seem to be the most likely sources of trouble, fat pads can also become inflamed, thick, stiff, and inelastic with a painfully similar outcome. (26,27)
3. Symptoms
Heel pad syndrome complaints are typically described as a deep, diffuse, nonspecific bruise-like pain localized at the center of the heel. (42) Patients may report tenderness to touch. Symptoms are typically exacerbated by walking on hard surfaces or barefoot, particularly for prolonged periods. (42,43)
4. Clinical Signs
The hallmark clinical feature of heel pad syndrome is tenderness to palpation at the center of the heel. (43) Springing palpation of a healthy heel pad should demonstrate significant elasticity. Loss of this springing elasticity suggests dysfunction.

Differentiating Heel Pad Syndrome from Plantar Fasciitis
Patients presenting with heel pad syndrome typically demonstrate centralized heel pain after prolonged activity, whereas plantar fasciitis patients experience medial calcaneal pain that is provoked upon initiation of activity. (18,52)
Clinicians should also inquire if symptoms improve when walking on their toes. Heel pad complaints typically improve with toe walking, whereas plantar fasciitis symptoms do not (aka Heel Pain Differentiation Maneuver). (88,89)

5. Heel Cups
Conservative management consists of offloading with relative rest and cushioning via padding or shoe modifications. (24,37) Cushioned heel cups are a mainstay of treatment (e.g., Tuli heel cup). (24,56-58) Heel cups can help dissipate pressure via weight redistribution. Heel cups can also help maintain proper positioning of the fat pad. (24,56,57)

6. Myofascial Release
Significant data shows that myofascial release techniques applied to the gastroc, soleus, and plantar fascia may reduce pain and improve function in plantar heel pain patients. (61-67)

7. Manipulation & Mobilization
Foot and ankle joint restrictions routinely contribute to heel pain. (48) Manipulation and mobilization of the foot and ankle joints may improve outcomes, although high-quality research support is lacking. (4,68)
8. Rehab
Stretching exercises should focus on restoring flexibility to the gastroc, soleus, and plantar fascia. (3,48,94) Proprioceptive exercises may help improve dynamic control of the foot and ankle.
Strengthening exercises should promote foot and ankle stability. Strengthening the toe flexors is an essential component of heel pain management. (91) Toe muscle rehab performed from a stretched position has been shown to improve strength by as much as 40%. (95) Peroneal muscle strengthening must not be overlooked. (91)
Check out one of our favorite exercises that incorporates several of these components:

9. Taping
Various taping techniques seek to dissipate force at the heel and limit foot hyperpronation. Therapeutic low-dye taping has shown merit in the management of heel pad syndrome. (69-71)

10. Medical Management
Medical management commonly includes anti-inflammatory medications. However, the value of steroid injections is questionable for plantar heel pain. (77) Repeated steroid injections can promote fat pad atrophy, thus are contraindicated. (57)
Summary
Manual therapists like you and me can easily be lulled into complacency by assuming that every heel pain presentation is plantar fasciitis. Recognizing the potential imposters for common diagnoses is essential for establishing our reputation as proficient providers. There’s a vast difference between merely treating someone and consistently applying best practices for the correct diagnosis. And in the future of healthcare, only the latter will be valued and reimbursed.
Did you know there’s also a difference between receiving this weekly blog and being part of the ChiroUp provider network? It’s like the difference between receiving the Mayo Clinic Newsletter and being a Mayo clinic provider. One’s a nice resource…but the other comes with countless additional benefits and privileges.
Access to 104 up-to-date best practice condition protocols with straightforward video tutorials of every associated test, treatment, exercise, and ADL – to help you nail down clinical excellence.
The ability to nearly instantly relay this information to patients via condition reports, like this one for Heel Pad Syndrome, that answers your patient’s essential questions plus video demonstrations of exercises and ADL’s -meaning better compliance with fewer questions.
Automated patient satisfaction and clinical outcome collection so you can see real-time feedback and know where and how to improve continually.
Automated Google and Healthgrades reviews from your most satisfied patients so you can market your most credible endorsements - high patient satisfaction and outcomes.
The confidence of being part of a network of evidence-based providers working together to continually refine best practices to become the undeniable best choice for patients and payors.
-
Buchbinder R. Plantar fasciitis. New England Journal of Medicine. 2004 May 20;350(21):2159-66. Link
Hossain M, Makwana N. “Not Plantar Fasciitis”: the differential diagnosis and management of heel pain syndrome. Orthopaedics and trauma. 2011 Jun 1;25(3):198-206.Link
Gaikwad P. Heel Fat Pad Syndrome Physiopedia. Accessed 04/18/2021 from: https://www.physio-pedia.com/Heel_Fat_Pad_Syndrome. Link
Hossain M, Makwana N. “Not Plantar Fasciitis”: the differential diagnosis and management of heel pain syndrome. Orthopaedics and trauma. 2011 Jun 1;25(3):198-206.Link
Crawford F, Thomson CE. Interventions for treating plantar heel pain. Cochrane Database of Systematic Reviews. 2003(3).Link
Chanda A, McClain S. Mechanical modeling of healthy and diseased calcaneal fat pad surrogates. Biomimetics. 2019 Mar;4(1):1.Link
Saad A, Kho J, Almeer G, Azzopardi C, Botchu R. Lesions of the heel fat pad. The British Journal of Radiology. 2021 Feb 1;94(1118):20200648.Link
Bordelon RL. Subcalcaneal pain. A method of evaluation and plan for treatment. Clinical orthopaedics and related research. 1983 Jul 1(177):49-53.Link
Ugbolue UC, Yates EL, Rowland KE, Wearing SC, Gu Y, Lam WK, Baker JS, Sculthorpe NF, Dutheil F. A novel simplified biomechanical assessment of the heel pad during foot plantarflexion. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2021 Feb;235(2):197-207.Link
Choo YJ, Park CH, Chang MC. Rearfoot disorders and conservative treatment: a narrative review. Annals of palliative medicine. 2020 Sep 1;9(5):3546-52.Link
Campanelli V, Fantini M, Faccioli N, Cangemi A, Pozzo A, Sbarbati A. Three-dimensional morphology of heel fat pad: an in vivo computed tomography study. Journal of anatomy. 2011;219(5):622–631. Link
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. 2020 Feb 6.Link
Jahss MH, Michelson JD, Desai P, Kaye R, Kummer F, Buschman W, Watkins F, Reich S. Investigations into the fat pads of the sole of the foot: anatomy and histology. Foot & ankle. 1992 Jun;13(5):233-42. Link
Ünlü RE, Orbay H, Kerem M, Esmer AF, Tüccar E, Şensöz Ö. Innervation of three weight-bearing areas of the foot: an anatomic study and clinical implications. Journal of plastic, reconstructive & aesthetic surgery. 2008 May 1;61(5):557-61.Link
Baxter DE, Thigpen CM. Heel pain—operative results. Foot & ankle. 1984 Jul;5(1):16-25.Link
Özdemır H, Söyüncü Y, Özgörgen M, Dabak K. Effects of changes in heel fat pad thickness and elasticity on heel pain. Journal of the American Podiatric Medical Association. 2004 Jan 1;94(1):47-52.Link
López López D, Becerro de Bengoa Vallejo R, Losa Iglesias ME, Soriano Medrano A, Palomo López P, Morales Ponce Á, Rodríguez Sanz D, Calvo Lobo C. Relationship between decreased subcalcaneal fat pad thickness and plantar heel pain. a case control study. Link
Im Yi T, Lee GE, Seo IS, Huh WS, Yoon TH, Kim BR. Clinical characteristics of the causes of plantar heel pain. Annals of rehabilitation medicine. 2011 Aug;35(4):507. Link
Jahss MH, Kummer F, Michelson JD. Investigations into the fat pads of the sole of the foot: heel pressure studies. Foot & ankle. 1992 Jun;13(5):227-32. Link
Hsu TC, Wang CL, Tsai WC, Kuo JK, Tang FT. Comparison of the mechanical properties of the heel pad between young and elderly adults. Archives of physical medicine and rehabilitation. 1998 Sep 1;79(9):1101-4.Link
Buschmann WR, Jahss MH, Kummer F, Desai P, Gee RO, Ricci JL. Histology and histomorphometric analysis of the normal and atrophic heel fat pad. Foot & Ankle International. 1995 May;16(5):254-8.Link
Hsu TC, Lee YS, Shau YW. Biomechanics of the heel pad for type 2 diabetic patients. Clinical Biomechanics. 2002 May 1;17(4):291-6.Link
Choo YJ, Park CH, Chang MC. Rearfoot disorders and conservative treatment: a narrative review. Annals of palliative medicine. 2020 Sep 1;9(5):3546-52.Link
Jahss MH, Michelson JD, Desai P, Kaye R, Kummer F, Buschman W, Watkins F, Reich S. Investigations into the fat pads of the sole of the foot: anatomy and histology. Foot & ankle. 1992 Jun;13(5):233-42. Link
Hsu TC, Wang CL, Tsai WC, Kuo JK, Tang FT. Comparison of the mechanical properties of the heel pad between young and elderly adults. Archives of physical medicine and rehabilitation. 1998 Sep 1;79(9):1101-4.Link
Özdemır H, Söyüncü Y, Özgörgen M, Dabak K. Effects of changes in heel fat pad thickness and elasticity on heel pain. Journal of the American Podiatric Medical Association. 2004 Jan 1;94(1):47-52.Link
Juliano PJ, Harris TG. Plantar fasciitis, entrapment neuropathies, and tarsal tunnel syndrome: current up to date treatment. Current Opinion in Orthopaedics. 2004 Apr 1;15(2):49-54.Link
Rome K, Webb P, Unsworth A, Haslock I. Heel pad stiffness in runners with plantar heel pain. Clinical Biomechanics. 2001 Dec 1;16(10):901-5.Link
Buschmann WR, Hudgins LC, Kummer F, Desai P, Jahss MH. Fatty acid composition of normal and atrophied heel fat pad. Foot & ankle. 1993 Sep;14(7):389-94.Link
Quirk R: Metatarsalgia. Aust Fam Phys. 1996;25(6):863-865.
Turgut A, Göktürk E, Köse N, Seber S, Hazer B, Günal Î. The relationship of heel pad elasticity and plantar heel pain. Clinical Orthopaedics and Related Research®. 1999 Mar 1;360:191-6.Link
Mann RA. Metatarsalgia: common causes and conservative treatment. Postgraduate medicine. 1984 Apr 1;75(5):150-67.Link
Resnick RB, Hudgins LC, Buschmann WR, Kummer FJ, Jahss MH. Analysis of the heel pad fat in rheumatoid arthritis. Foot & ankle international. 1999 Aug;20(8):481-4. Link
Rocchio TM. Augmentation of atrophic plantar soft tissue with an acellular dermal allograft: a series review. Clinics in podiatric medicine and surgery. 2009 Oct 1;26(4):545-57.Link
Kao PF, Davis BL, Hardy PA. Characterization of the calcaneal fat pad in diabetic and non-diabetic patients using magnetic resonance imaging. Magnetic resonance imaging. 1999 Jul 1;17(6):851-7. Link
Joseph Vella DP, Schleicher S. Expert Insights On Therapies For Plantar Fat Pad Atrophy. 2015 May 28. Link
Falsetti P, Frediani B, Acciai C, Baldi F, Filippou G, Marcolongo R. Heel fat pad involvement in rheumatoid arthritis and in spondyloarthropathies: an ultrasonographic study. Scandinavian journal of rheumatology. 2004 Oct 1;33(5):327-31.Link
Belhan O, Kaya M, Gurger M. The thickness of heel fat-pad in patients with plantar fasciitis. Acta orthopaedica et traumatologica turcica. 2019 Nov 1;53(6):463-7.Link
Hossain M, Makwana N. “Not Plantar Fasciitis”: the differential diagnosis and management of heel pain syndrome. Orthopaedics and trauma. 2011 Jun 1;25(3):198-206.Link
Natali AN, Fontanella CG, Carniel EL. A numerical model for investigating the mechanics of calcaneal fat pad region. Journal of the Mechanical Behavior of Biomedical Materials. 2012 Jan 1;5(1):216-23.Link
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. 2020 Feb 6. Link
Choo YJ, Park CH, Chang MC. Rearfoot disorders and conservative treatment: a narrative review. Annals of palliative medicine. 2020 Sep 1;9(5):3546-52. Link
Landorf KB, Radford JA. Minimal important difference: values for the foot health status questionnaire, foot function index and visual analogue scale. The Foot. 2008 Mar 1;18(1):15-9. Link
Martin RL, Irrgang JJ, Burdett RG, Conti SF, Swearingen JM. Evidence of validity for the Foot and Ankle Ability Measure (FAAM). Foot & Ankle International. 2005 Nov;26(11):968-83.Link
Binkley JM, Stratford PW, Lott SA, Riddle DL, North American Orthopaedic Rehabilitation Research Network. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. Physical therapy. 1999 Apr 1;79(4):371-83. Link
Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a systematic review. Journal of science and medicine in sport. 2006 May 1;9(1-2):11-22.Link
Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: a matched case-control study. JBJS. 2003 May 1;85(5):872-7. Link
Van Hul E, Vanhoenacker F, Van Dyck P, De Schepper A, Parizel PM. Pseudotumoural soft tissue lesions of the foot and ankle: a pictorial review. Insights into imaging. 2011 Aug;2(4):439-52. Link
Belhan O, Kaya M, Gurger M. The thickness of heel fat-pad in patients with plantar fasciitis. Acta orthopaedica et traumatologica turcica. 2019 Nov 1;53(6):463-7. Link
Saad A, Kho J, Almeer G, Azzopardi C, Botchu R. Lesions of the heel fat pad. The British Journal of Radiology. 2021 Feb 1;94(1118):20200648.Link
Im Yi T, Lee GE, Seo IS, Huh WS, Yoon TH, Kim BR. Clinical characteristics of the causes of plantar heel pain. Annals of rehabilitation medicine. 2011 Aug;35(4):507.Link
Hossain M, Makwana N. “Not Plantar Fasciitis”: the differential diagnosis and management of heel pain syndrome. Orthopaedics and trauma. 2011 Jun 1;25(3):198-206.Link
Martin RL, Davenport TE, Reischl SF, McPoil TG, Matheson JW, Wukich DK, McDonough CM, Altman RD, Beattie P, Cornwall M, Davis I. Heel pain—plantar fasciitis: revision 2014. Journal of Orthopaedic & Sports Physical Therapy. 2014 Nov;44(11):A1-33. Link
Rosenbaum AJ, DiPreta JA, Misener D. Plantar heel pain. Medical Clinics. 2014 Mar 1;98(2):339-52.Link
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. 2020 Feb 6.Link
Rose B, Singh D. Inferior heel pain. Orthopaedics and Trauma. 2020 Feb 1;34(1):10-6.Link
Chanda A, McClain S. Mechanical modeling of healthy and diseased calcaneal fat pad surrogates. Biomimetics. 2019 Mar;4(1):1. Link
Rasenberg N, Riel H, Rathleff MS, Bierma-Zeinstra SM, van Middelkoop M. Efficacy of foot orthoses for the treatment of plantar heel pain: a systematic review and meta-analysis. British journal of sports medicine. 2018 Aug 1;52(16):1040-6.Link
Taheri A, Jafarian FS, Sadeghi-Demneh E, Bahmani F. The effects of foot orthoses on pain management of people with plantar fasciitis. Clinical Research on Foot & Ankle. 2015 Sep 26:1-5.Link
Kuhar S, Subhash K, Chitra J. Effectiveness of myofascial release in treatment of plantar fasciitis: A RCT. Indian J Physiother Occup Ther. 2007 Apr;1(3):3-9. Link
Yadav AO, Lakshmiprabha R. Comparison of the effects of therapeutic ultrasound v/s myofascial release technique in treatment of plantar fasciitis. Indian J Physiother Occup Ther. 2012 Apr;6(2):13-6.Link
Renan-Ordine R, Alburquerque-SendÍn F, Rodrigues De Souza DP, Cleland JA, Fernández-De-Las-Penas C. Effectiveness of myofascial trigger point manual therapy combined with a self-stretching protocol for the management of plantar heel pain: a randomized controlled trial. journal of orthopaedic & sports physical therapy. 2011 Feb;41(2):43-50.Link
Ajimsha MS, Binsu D, Chithra S. Effectiveness of myofascial release in the management of plantar heel pain: a randomized controlled trial. The Foot. 2014 Jun 1;24(2):66-71.Link
Dimou ES, Brantingham JW, Wood T. A randomized, controlled trial (with blinded observer) of chiropractic manipulation and Achilles stretching vs. orthotics for the treatment of plantar fasciitis. Journal of the American Chiropractic Association. 2004 Sep 1;41(9).Link
Cleland JA, Abbott JH, Kidd MO, Stockwell S, Cheney S, Gerrard DF, Flynn TW. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: a multicenter randomized clinical trial. journal of orthopaedic & sports physical therapy. 2009 Aug;39(8):573-85. Link
Saban B, Deutscher D, Ziv T. Deep massage to posterior calf muscles in combination with neural mobilization exercises as a treatment for heel pain: a pilot randomized clinical trial. Manual therapy. 2014 Apr 1;19(2):102-8. Link
Dimou ES, Brantingham JW, Wood T. A randomized, controlled trial (with blinded observer) of chiropractic manipulation and Achilles stretching vs. orthotics for the treatment of plantar fasciitis. Journal of the American Chiropractic Association. 2004 Sep 1;41(9). Link
Yi TI, Shim JW, Ku HK, Seo IS, Huh WS, Kim JS, Park JS. The Effects of Modified Low-Dye Taping in the Patient with Heel Pad Atrophy. Journal of the Korean Academy of Rehabilitation Medicine. 2011 Feb 1;35(1):96-100.Link
Ha HS, Hwang JH, Kim YB, Ha YM, Hwang JM. Immediate clinical and biomechanical effects of low-dye taping in patients with plantar heel pain. The Korean Journal of Sports Medicine. 2012 Jun 1;30(1):9-15. Link
Chae YH, Kim JS, Kang Y, Kim HY, Im Yi T. Clinical and biomechanical effects of low-dye taping and figure-8 modification of low-dye taping in Patients with heel pad atrophy. Annals of rehabilitation medicine. 2018 Apr;42(2):222.Link
Radford JA, Burns J, Buchbinder R, Landorf KB, Cook C. The effect of low-dye taping on kinematic, kinetic, and electromyographic variables: a systematic review. Journal of Orthopaedic & Sports Physical Therapy. 2006 Apr;36(4):232-41.Link
Newell T, Simon J, Docherty CL. Arch-taping techniques for altering navicular height and plantar pressures during activity. Journal of athletic training. 2015 Aug;50(8):825-32. Link
Schoenhaus J. Treating Fat Pad Atrophy. Podiatry Today. April 03, 2017. Link
Balkin SW. Injectable silicone and the foot: a 41‐year clinical and histologic history. Dermatologic surgery. 2005 Nov;31:1555-60.Link
Gusenoff JA, Mitchell RT, Jeong K, Wukich DK, Gusenoff BR. Autologous fat grafting for pedal fat pad atrophy: a prospective randomized clinical trial. Plastic and reconstructive surgery. 2016 Nov 1;138(5):1099-108.Link
Whittaker GA, Munteanu SE, Menz HB, Bonanno DR, Gerrard JM, Landorf KB. Corticosteroid injection for plantar heel pain: a systematic review and meta-analysis. BMC musculoskeletal disorders. 2019 Dec 1;20(1):378. Link
Liao CD, Tsauo JY, Chen HC, Liou TH. Efficacy of Extracorporeal Shock Wave Therapy for Lower-Limb Tendinopathy: A Meta-analysis of Randomized Controlled Trials. American journal of physical medicine & rehabilitation. 2018 Sep 1;97(9):605-19. Link
Mishra BN, Poudel RR, Banskota B, Shrestha BK, Banskota AK. Effectiveness of extra-corporeal shock wave therapy (ESWT) vs methylprednisolone injections in plantar fasciitis. Journal of clinical orthopaedics and trauma. 2019 Mar 1;10(2):401-5. Link
Sanmak ÖD, Külcü DG, Mesci N, Altunok EÇ. Comparison of effects of low-level laser therapy and extracorporeal shock wave therapy in plantar fasciitis treatment: A randomized, prospective, single-blind clinical study. Turkish Journal of Physical Medicine and Rehabilitation. 2019 Jun;65(2):184. Link
Sun K, Zhou H, Jiang W. Extracorporeal shock wave therapy versus other therapeutic methods for chronic plantar fasciitis. Foot and Ankle Surgery. 2020 Jan 1;26(1):33-8.Link
Xu D, Jiang W, Huang D, Hu X, Wang Y, Li H, Zhou S, Gan K, Ma W. Comparison Between Extracorporeal Shock Wave Therapy and Local Corticosteroid Injection for Plantar Fasciitis. Foot & ankle international. 2019 Nov 19:1071100719891111. Link
Al-Abbad H, Allen S, Morris S, Reznik J, Biros E, Paulik B, Wright A. The effects of shockwave therapy on musculoskeletal conditions based on changes in imaging: a systematic review and meta-analysis with meta-regression. BMC Musculoskeletal Disorders. 2020 Dec;21(1):1-26. Link
Mitchkash M, Robinson D, Tenforde A. Efficacy of Extracorporeal Pulse-Activated Therapy in the Management of Lower-Extremity Running-Related Injuries: Findings From a Large Case Cohort. The Journal of Foot and Ankle Surgery. 2020 Apr 25. Link
Sanmak ÖD, Külcü DG, Mesci N, Altunok EÇ. Comparison of effects of low-level laser therapy and extracorporeal shock wave therapy in plantar fasciitis treatment: A randomized, prospective, single-blind clinical study. Turkish Journal of Physical Medicine and Rehabilitation. 2019 Jun;65(2):184. Link
Irving DB, Cook JL, Young MA, Menz HB. Obesity and pronated foot type may increase the risk of chronic plantar heel pain: a matched case-control study. BMC musculoskeletal disorders. 2007 Dec;8(1):1-8. Link
Katoh Y, Chao EY, Morrey BF, Laughman RK. Objective technique for evaluating painful heel syndrome and its treatment. Foot & ankle. 1983 Jan;3(4):227-36.Link
Michaud TC. RE: “Heel Pad Syndrome Protocol.” Message to Tim Bertelsman regarding advice on chiropractic management of heel pad syndrome patients via direct email on 04/22/2021.
Michaud TC. Human locomotion: the conservative management of gait-related disorders. pp. 95-97. Newton Biomechanics; 2011.
De Clercq D, Aerts P, Kunnen M. The mechanical characteristics of the human heel pad during foot strike in running: an in vivo cineradiographic study. Journal of biomechanics. 1994 Oct 1;27(10):1213-22.Link
Michaud TC. Managing Heel Pain: The Overlooked Role of Peroneal and Toe Flexor Strength Accessed fromwww.HumanLocomotion.com on 04/22/21Link
Whittaker GA, Munteanu SE, Menz HB, Tan JM, Rabusin CL, Landorf KB. Foot orthoses for plantar heel pain: a systematic review and meta-analysis. British journal of sports medicine. 2018 Mar 1;52(5):322-8. Link
Sullivan J, Burns J, Adams R, Pappas E, Crosbie J. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot & ankle international. 2015 Jan;36(1):37-45.Link
DiGiovanni BF, Nawoczenski DA, Lintal ME, Moore EA, Murray JC, Wilding GE, Baumhauer JF. Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain: a prospective, randomized study. JBJS. 2003 Jul 1;85(7):1270-7.Link
Goldmann JP, Sanno M, Willwacher S, Heinrich K, Brüggemann GP. The potential of toe flexor muscles to enhance performance. Journal of sports sciences. 2013 Feb 1;31(4):424-33.Link