
Chiropractic Treatment of Diabetes
Why Chiropractors Must Understand Patients with Diabetes
While many chiropractors typically focus solely on musculoskeletal diagnoses, this blog challenges the status quo. Health professionals must grasp the intricate connection between metabolic disorders and muscular ailments. One such common metabolic disorder that significantly influences clinical care is DIABETES. After reading this blog, you will gain the following:
Gain insights into how this metabolic disease directly impacts the musculoskeletal system.
Uncover simple yet effective tips to identify when diabetes may affect your clinical care.
Then, equip yourself with valuable treatment strategies to facilitate recovery for these patients.
How does diabetes affect your patients?
Diabetes mellitus (DM) affects connective tissues causing alterations in periarticular and skeletal tissue. (1) Surprisingly, abnormalities of the lower extremities are not as common as disorders affecting the hands and shoulders secondary to DM. Here are three complications of DM that affect your patients:
Stiffer Joints
Diabetes causes stiff joints due to abnormal collagen deposition after injury. Newly formed collagen is thickened and disorganized, preventing sliding between tendon/ligament surfaces. (2) Long-standing joint and tendon injury also increases the incidence of calcific changes at the place where tendons attach to bones within the diabetic population.
This study demonstrated that patients with DM had a 27% increased risk of developing calcific tendinopathy of the shoulder." (3)
Reduced Blood Flow
Microvascular disease secondary to diabetes can be the result or cause of a musculoskeletal disorder. Prolonged high blood glucose levels can damage the walls of blood vessels leading to a reduced ability of blood vessels to dilate and constrict properly, thereby affecting blood flow. This reduction in blood flow is another variable leading to reduced healing time within your patient population.
Weaker Tissue
There is a clear connection between diabetes and a higher risk of fractures and difficulties in healing bone, ligament, and muscle injuries. This link is partly due to the non-enzymatic glycosylation of collagen molecules, which creates advanced glycation end products (AGEs). Collagen is a crucial component of connective tissues like ligaments, tendons, and bones. AGEs weaken collagen's structure and biomechanical properties, resulting in weaker tissues. (4)
If the treatment of diabetes falls outside of your SCOPE or EXPERTISE, you must still follow up with our patients concerning their diabetes. DM affects their health and our clinical success while treating other conditions.
3 Conditions Secondary to Diabetes
Dupuytren’s disease (DD) is a spontaneously occurring chronic and idiopathic thickening of the palmar aponeurosis leading to various degrees of flexion deformity of the fingers. (5) Diabetic patients suffer from DD due to ineffective tissue repair after injury to the hand's tendons.
Carpal Tunnel Syndrome (CTS) also seems more frequent in diabetic subjects than in the general population. CTS appears to be more a neuropathic than an entrapment disorder in diabetics, although connective tissue stiffening and overgrowth could contribute to nerve compression. (6) Phalen reported that DM was the most common systemic disease associated with CTS in 63 of 379 (17%) patients. (7)
Nerve flossing may help keep the nerve mobile and healthy during your treatment plan!

Adhesive Capsulitis (AC) results in pain and increasing shoulder stiffness. (8) DM accelerates the fundamental pathological changes seen in AC. These patients have thickening of the joint capsule and adherence of the capsule to the head of the humerus. Histological and histochemical studies indicate that this abnormal fibrotic process causes capsular contracture resulting in AC. (9)
Chiropractic Treatment of Diabetes
1. Avoid Steroids
Using oral and injectable steroids may lead to hyperglycemia, amplifying the adverse side effects of DM. (1)

2. Extend your treatment plan.
After an injury, the average healing rate of the tendon is approximately 1% per day. Healing time is modifiable by biological sex and excessive load after damage. However, other variables SLOW healing time, like diabetes mellitus. (10)
3. Fast Walking
Diabetic subjects present gait features including: (11)
Increased step width
Reduced step and stride length, and walking velocity
Reduction in ankle plantarflexion during the push-off phase
Reduced peak knee flexion during the swing time of the gait cycle
Gait retraining, walking faster, and increasing vigorous physical activity to at least 20 minutes per day are helpful nonpharmaceutical interventions to improve quality of life. (12)
Download this ChiroUp infographic to deliver information on walking to your patients!

4. Reduce diabetic neuropathy pain.
"The findings of this review suggested incorporating an exercise program for painful diabetic neuropathy. Exercise intervention is effective in reducing the Michigan neuropathy score." (13) Your patients with diabetic neuropathy often complain of widespread and diffuse pain. Creating and implementing an exercise program for these patients will reduce symptoms.
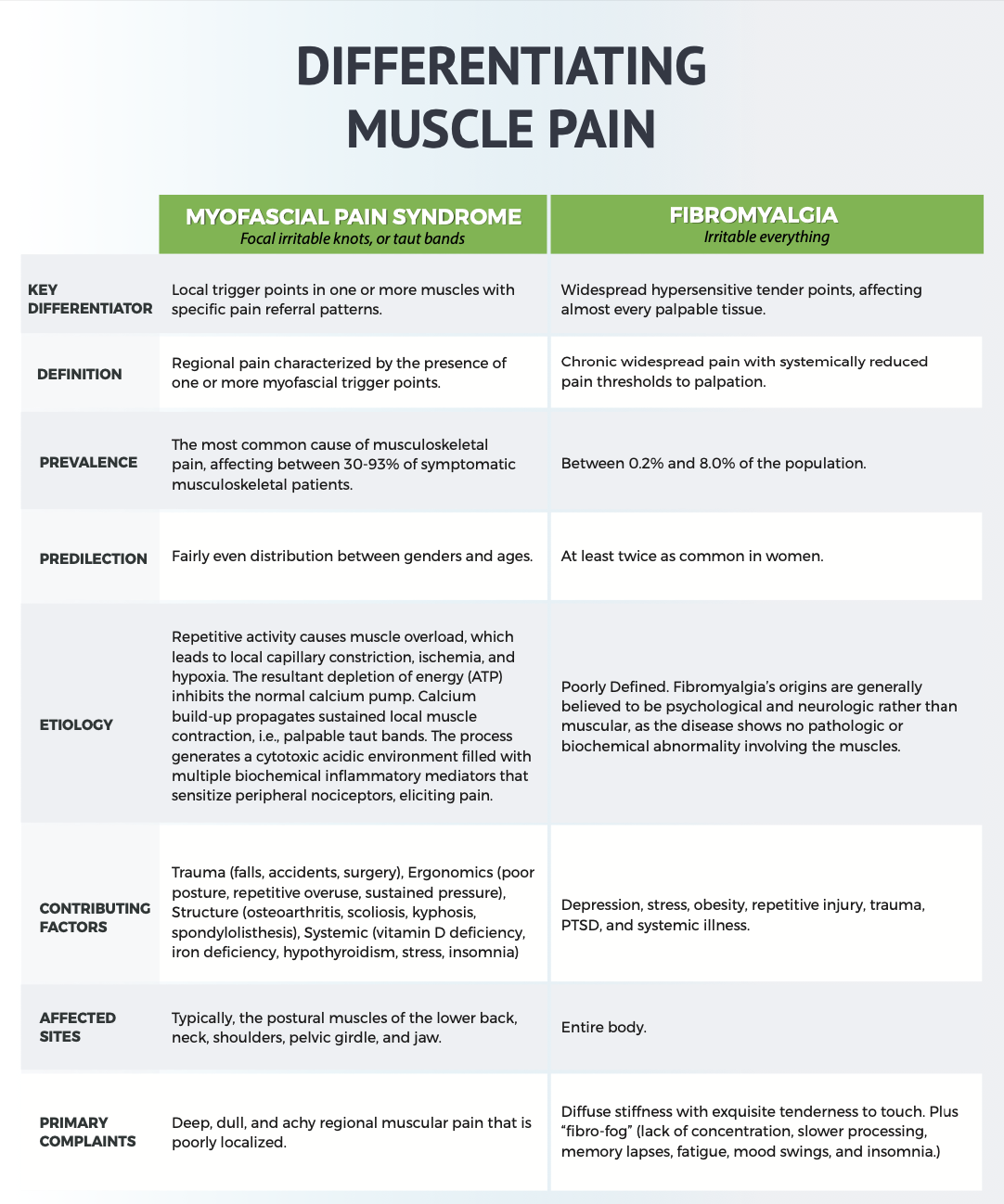
5. Fibromyalgia or Undiagnosed DM
Many patients with fibromyalgia (FM) may also suffer from MSK pain due to undiagnosed diabetes. Impaired glucose regulation seen in FM patients may be due to DM. Astute providers should test FM patients for possible co-morbid diabetes. (14)
ChiroUp subscribers can download the following infographic in the Forms Library by searching “Myofascial”. Not yet a subscriber? Sign up now for FREE.
6. Nutritional Advice
Incorporating advice for meal timing with prolonged fasting can improve glucose metabolism. (15) Also, consider giving your patients this infographic to reduce A1C levels if they already have diabetes or looking to reduce to incidence of developing diabetes.
ChiroUp subscribers can download the following infographic to deliver to their parents in the Forms Library by searching “Nutrition”. Not yet a subscriber? Sign up now for FREE.

7. Refer Out
If treating diabetes is not your expertise, refer to someone that can help. Many functional medicine physicians, chiropractors, and medical doctors make this their life work. Find someone in your area who can help your patient improve their health.
In closing, we want to acknowledge the dedication and commitment of health professionals like you who tirelessly strive to understand the complexities of metabolic disorders, muscular ailments, and the multitude of clinical conditions that chiropractors can treat. We recognize the challenges you face in staying up-to-date with the latest research and treatment options.
At ChiroUp, we are here to support you on your journey to excellence. Our platform empowers you with immediate access to the most current, evidence-based research, allowing you to diagnose and treat over 100 conditions with confidence.
Your patients deserve the very best. YOU are the right doc to provide that.
Join our network today. ChiroUp providers are making a difference in the lives of countless individuals, and together, we are shaping the future of chiropractic care.
-
Arkkila, P. E., & Gautier, J.-F. (2003). Musculoskeletal disorders in diabetes mellitus: an update. Best Practice & Research Clinical Rheumatology, 17(6), 945–970. doi:10.1016/j.berh.2003.11.001
Vaidya R, Lake SP, Zellers JA. Effect of Diabetes on Tendon Structure and Function: Not Limited to Collagen Crosslinking. Journal of Diabetes Science and Technology. 2022 Jun 2:19322968221100842.
Su YC, Chung CH, Ke MJ, Chen LC, Chien WC, Wu YT. Increased risk of shoulder calcific tendinopathy in diabetes mellitus: a nationwide, population-based, matched cohort study. International Journal of Clinical Practice. e14549. Link
Stolarczyk A, Sarzyńska S, Gondek A, Cudnoch‐Jędrzejewska A. Influence of diabetes on tissue healing in orthopedic injuries. Clinical and Experimental Pharmacology and Physiology. 2018 Jul;45(7):619-27.
Dupuytren G. Permanent retraction of the fingers, produced by an affection of the palmar fascia. Lancet 1834; ii: 222–225.
Jung Y, Hohmann TC, Gerneth JA et al. Diabetic hand syndrome. Metabolism 1971; 20: 1008–1015.
Phalen GS. Reflections on 21 years of experience with carpal tunnel syndrome. JAMA 1970; 212: 1365–1367
Duplay S. De la pe´ri-arthrite scapulo-hume´rale et des raideurs de l’e´paule qui en sont la conse´quence. Archives Ge´ne´rates de Me´decine 1872; 20: 513–542.
Fisher L, Kurtz A & Shipley M. Association between neuroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. British Journal of Rheumatology 1986; 25: 141–146
Griffith KM, Hammer LC, Iannuzzi NP, Takatani KC, Hsu JE, Cotton JD, Gee AO, Gardner RJ, Lack WD. Review of human supraspinatus tendon mechanics part II: Tendon healing response and characterization of tendon health. Journal of Shoulder and Elbow Surgery. 2022 Jul 5.
Tramonti C, Iacopi E, Cavalli M, Riitano N, Piaggesi A, Chisari C. Type 2 diabetes mellitus and obesity: The synergistic effects on human locomotor function. Clinical Biomechanics. 2022 Dec 1;100:105759.
Cochrane SK, Chen SH, Fitzgerald JD, Dodson JA, Fielding RA, King AC, McDermott MM, Manini TM, Marsh AP, Newman AB, Pahor M. Association of accelerometry measured physical activity and cardiovascular events in mobility limited older adults: the life (lifestyle interventions and independence for elders) study. Journal of the American Heart Association. 2017 Dec 2;6(12):e007215.
Tatikola SP, Natarajan V, Desai VK, Asirvatham AR, Rajsekhar H. Effect of various exercise protocols on neuropathic pain in individuals with type 2 diabetes with peripheral neuropathy: A systematic review and meta-analysis. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2022 Aug 27:102603.
Zetterman T, Markkula R, Kalso E. Glucose tolerance in fibromyalgia. Medicine. 2021 Nov 19;100(46).
Teong, X.T., Liu, K., Vincent, A.D., et al. Intermittent fasting plus early time-restricted eating versus calorie restriction and standard care in adults at risk of type 2 diabetes: a randomized controlled trial. Nat Med 29, 963–972 (2023). https://doi.org/10.1038/s41591-023-02287-7