
Chiropractic Management of Coccydynia
Reading time: 5 minutes
Coccydynia originates from various traumatic and non-traumatic factors. Many cases resolve spontaneously; others can lead to chronic and potentially debilitating pain syndromes. (1) Patients and providers often ignore the problem since management may involve intrarectal assessment and management.
Fortunately, your ChiroUp team has recently compiled an up-to-date, best practice protocol for managing this troublesome complaint. Check out our top clinical pearls:
Coccydynia Etiology
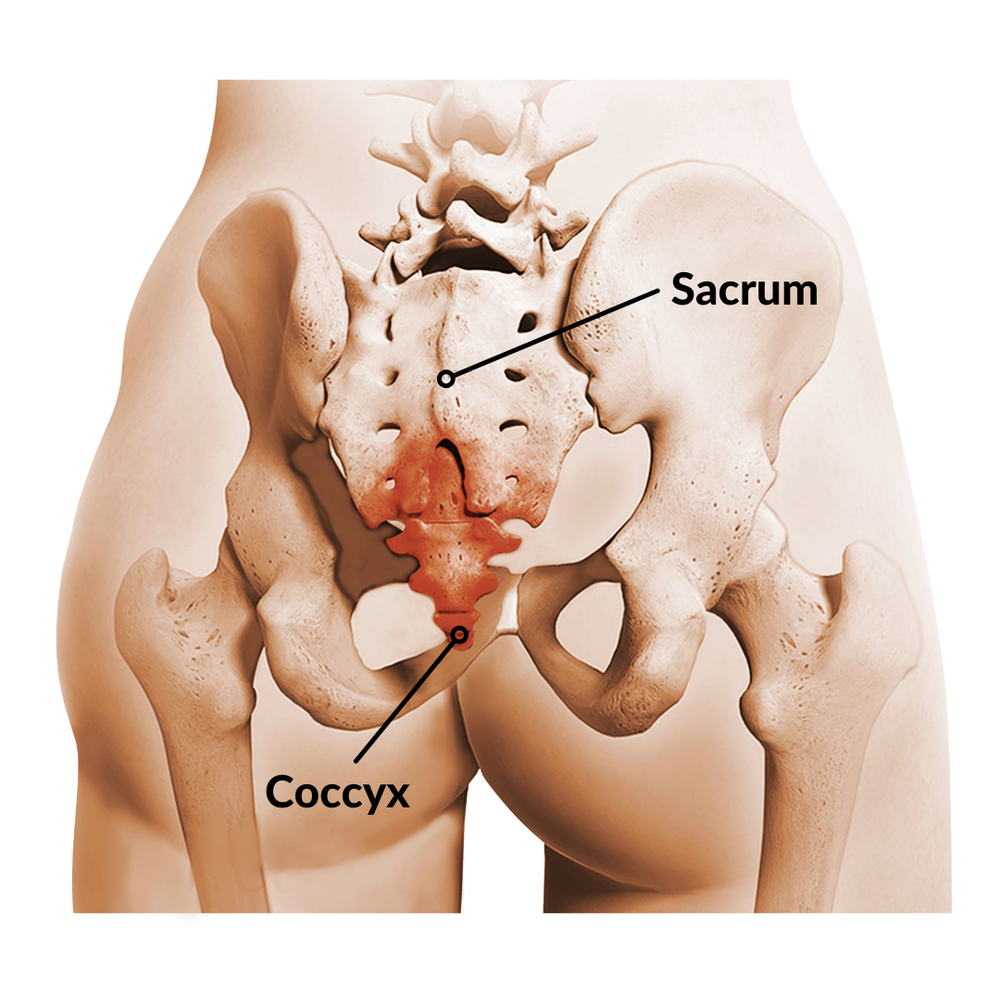
Coccydynia symptoms can arise from many etiologies, including bruised or broken coccygeal segments, chronic myofascial irritation, and sacrococcygeal joint dysfunction, degeneration, or dislocation. Traumatic etiologies are more common than insidious onsets and can have many triggers:
Acute external trauma from a backward fall onto the buttocks (7)
Acute internal trauma during childbirth.
Chronic external trauma from prolonged sitting on hard or narrow seats (15)
Chronic internal trauma from repetitive straining for bowel movements or intercourse (70)
Repeated impact exercise (73)
Coccydynia Presenting Complaints
The classic coccydynia presentation includes:
Localized "tailbone pain” provoked by activity.
A "constant deep ache" that becomes acute, sharp, or shooting upon movement.
Worse when sitting, particularly when reclining backward. (16,17)
Increased pain arising from a seated position due to contraction from the gluteus maximus. (16,17)
Sexual intercourse and defecation can sometimes intensify discomfort. (70)
Coccydynia General Assessment

The goal of chiropractic coccydynia assessment is first to rule out bony pathology (fracture, dislocation) and then identify any contributions from soft tissues (myofascial pain, sprain/ strain) and joints (hypermobility vs. hypomobility).
Tenderness to palpation is the hallmark clinical finding of coccydynia. (20-23)
Direct palpation can help differentiate local versus referred sources of coccydynia, which do not typically include coccygeal point tenderness or swelling. (1)
Radiographs may be appropriate to help identify degenerative changes and rule out dislocation or fracture, particularly following traumatic onsets. (34,35)
Coccydynia Orthopedic Tests
Coccydynia orthopedic evaluation aims to provoke coccygeal pain via compression or traction.

Foye's finger test is a simple assessment to help differentiate sacrococcygeal versus lumbosacral or sacroiliac pain. The patient is asked to use one finger to point to their most intense site of pain. Pointing to the midline of the tailbone suggests coccygeal involvement. (26)

The seated recline test begins with the patient sitting upright on a firm surface and then rolling backward 30 to 45 degrees to transition weight from the ischial tuberosities onto the coccyx; reproduction of tailbone pain suggests coccygeal involvement.
⚠️ Coccydynia Internal Assessment Concerns
Manual therapists should carefully consider whether they are the best-suited clinician for internal hands-on coccygeal assessment and treatment. Before embarking on any internal palpatory evaluation, examiners must weigh many factors, including:
Scope Of Practice Laws
Training
Informed Consent
Patient Expectations
Gender Preferences
Liability Issues
Experts advise extreme caution by obtaining a signed and witnessed informed consent that clearly outlines the procedure and rationale, utilizing a professional chaperone/ observer during treatment, plus offering the opportunity for the patient to have an additional family member with them during treatment. Providers should also document each aspect of care, including their clinical justification for the assessment or procedure. (72)
Coccydynia Internal Rectal Examination
Some clinicians choose to perform an internal rectal examination of the coccyx to assess for tenderness and hypermobility or hypomobility of the sacrococcygeal joint and myofascial involvement. (1,22,23,29,71)

To perform an internal sacrococcygeal joint assessment, the clinician pinches the patient's coccyx between their internal finger and external thumb, then assesses mobility in flexion and extension. Normal motion varies between 5 and 15 degrees in either direction. (30-32) Lateral flexion and rotation motion can also be assessed. (73) Acute presentations may have difficulty tolerating internal assessment. (23)
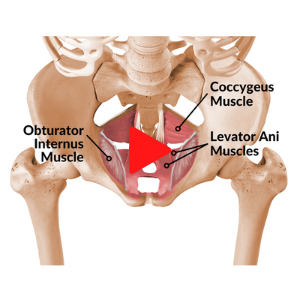
The internal coccygeal myofascial examination would typically include a trigger point assessment of the levator ani, coccygeus, and obturator internus muscles via a 360-degree clock-like sweep to identify areas of local sensitivity or hypertonicity. (19,29,33). Clinicians will frequently identify one or more internal trigger points that reproduce the patient’s specific complaint. (33)
Want More Detail?
ChiroUp subscribers can visit their in-app Condition Reference tab to review the complete Coccydynia protocol (or any of the other 110 protocols), including all associated assessments, treatments, and exercise videos.
Not yet a subscriber? Try it now for FREE!
Other Joints and Muscles
Coccydynia evaluation should include careful consideration of referral from lumbosacral or sacroiliac contributors. (23,29)
Chronic leaning toward one side to unload the tender coccyx while sitting can shorten the quadratus lumborum, TFL, iliopsoas, or piriformis. (71)
Clinicians should screen for potential concurrent functional deficits, including dysfunctional breathing, pelvic floor dysfunction, hip abductor weakness, and foot hyperpronation.
Coccydynia Treatment Considerations
Coccydynia is a common condition that can prove challenging to treat. (1,34) Fortunately, 90% of coccydynia cases can be resolved via straightforward conservative management. (38-40) Chiropractic coccydynia management decisions are based on etiological factors.
Acute presentations may benefit from relative rest, inflatable cushions, stool softeners, and NSAIDs, while chronic cases may benefit from myofascial release techniques. (41)
Gentle repositioning may be appropriate for acute trauma, mobilization may be appropriate for hypomobility, and myofascial release is best suited for addressing soft tissue origins. (19,42)
Coccydynia External Manipulation
Various authors have reported success with external manual or instrument-assisted manipulation/mobilization of the coccyx and sacroiliac joints. (43-45) Spinal manipulation should be considered for joint mobility deficits in the spine or pelvis.

Coccydynia Internal Manipulation Techniques

Intrarectal manipulation of the sacrococcygeal joint has shown merit. (25,47-50) Internal coccygeal manipulation is performed by grasping the patient's coccyx between the clinician’s internal finger and external thumb, then applying a gentle posterior pull to move the coccyx and sacrococcygeal joint into extension. (19,25,29,50,51) Extension over-pressure may be maintained for several seconds. (25) Gentle mobilization/ repositioning is performed once to reduce unstable fractures or dislocations and up to three repetitions per treatment session for more chronic and stable hypomobile presentations. (29)

Internal myofascial release of the levator ani, coccygeal, and obturator internus can be performed via a slow, internal 360-degree clock-like sweep to identify areas of local sensitivity or hypertonicity. The release is performed by applying 15 to 20 seconds of tolerable sustained compression over any identified trigger points. (19,33,50,52) External massage of the pericoccygeal muscles may also be helpful. (50,69)
Coccydynia Rehab Exercises
Clinicians should address the external muscles that impact coccygeal function, including the gluteus maximus, hamstrings, iliopsoas, and piriformis. (53,54) Additional mobility exercises could include posterior pelvic tilt and knee to chest. Exercises including the dead bug, bird dog, side bridge, and modified planks (on hands and toes, lift knees) progressing to planks may help improve core stability.

Supine Piriformis Stretch

Posterior Pelvic Tilt Standing

Knee to Chest
Coccydynia Treatment Expectations
Manual therapy, including massage, stretching, mobilization, and manipulation, has demonstrated positive clinical outcomes. (25,34,41,47-49,55,56)
Three sessions of intrarectal coccygeal manual therapy have a reported long-term success rate between 24 to 43%. (25,49,57,58)
Appropriate manual therapy typically produces results within 1-3 visits. (19,29)
Positive treatment prognosticators for manual therapy include a recent post-traumatic onset with relatively normal coccygeal mobility. (25,49)
Patients with coccygeal instability or immobility have lower success rates. (58)
Coccydynia ADL Considerations
Patients should consider using a modified wedge-shaped cushion to relieve coccygeal pressure while sitting. Patients should choose a U-shaped pillow over circular varieties, which place undesired pressure on the coccyx. (1) Other home advice includes:
Minimize prolonged sitting, particularly on hard or narrow seats, i.e., bicycles, motorcycles, horses, canoes, etc. (15,23,61)
Avoid sit-ups that can place an excessive mechanical load on the coccyx. (53)
Sit leaning slightly forward, thereby transitioning weight from the coccyx onto the ischial tuberosities.
A standing desk is often desirable.
Walking, swimming, and yoga may provide benefits for coccydynia patients. (53)
Maintain an optimal weight while avoiding excessively rapid weight loss. (62)
Temporarily avoid sexual positions that provoke symptoms.
Adequate fiber and water intake may help mitigate problems associated with constipation.
Avoid overly tight clothing.
Coccydynia Patient Education
This one is simple…Watch the video to see how simple with ChiroUp.
Download the ChiroUp Condition Report for Coccydynia
Like what you see? Create reports like these in less than 4 clicks for your patients! Our subscribers have greater than 80% average improvement within 30 days. Sounds amazing, right!? Get started with ChiroUp today to start seeing results like this.
*ChiroUp would like to thank Dr. James Lehman and Dr. Jeff Tucker who provided extensive content and professional direction for this protocol.
-
1. Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner Journal. 2014 Mar 20;14(1):84-7. Link
2. Mostafa E, Varacallo M. Anatomy, Back, Coccygeal Vertebrae. Link
3. Tague RG. Fusion of coccyx to sacrum in humans: prevalence, correlates, and effect on pelvic size, with obstetrical and evolutionary implications. American journal of physical anthropology. 2011 Jul;145(3):426-37. Link
4. Tetiker H, Koşar Mİ, Çullu N, Canbek U, Otağ I, Taştemur Y. MRI-based detailed evaluation of the anatomy of the human coccyx among Turkish adults. Nigerian Journal of Clinical Practice. 2017;20(2):136-42. Link
5. Maigne JY, Guedj S, Straus C. Idiopathic coccygodynia. Lateral roentgenograms in the sitting position and coccygeal discography. Spine. 1994 Apr 1;19(8):930-4. Link
6. Postacchini FR, Massobrio MA. Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. The Journal of bone and joint surgery. American volume. 1983 Oct 1;65(8):1116-24. Link
7. Nathan ST, Fisher BE, Roberts CS. Coccydynia: a review of pathoanatomy, aetiology, treatment and outcome. The Journal of bone and joint surgery. British volume. 2010 Dec;92(12):1622-7. Link
8. Woon JT, Stringer* MD. Redefining the coccygeal plexus. Clinical Anatomy. 2014 Mar;27(2):254-60. Link
9. Cramer GD, Ro CS. The sacrum, sacroiliac joint, and coccyx. Clinical Anatomy of the Spine, Spinal Cord, and Ans. 2014 Jan 1:312-39. Link
10. Maigne JY, Pigeau I, Aguer N, Doursounian L, Chatellier G. Chronic coccydynia in adolescents. A series of 53 patients. European journal of physical and rehabilitation medicine. 2011 Jun;47(2):245-51. Link
11. Maigne JY, Doursounian L, Chatellier G. Causes and mechanisms of common coccydynia: role of body mass index and coccygeal trauma. Spine. 2000 Dec 1;25(23):3072-9. Link
12. Fogel GR, Cunningham III PY, Esses SI. Coccygodynia: evaluation and management. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2004 Jan 1;12(1):49-54. Link
13. De Andrés J, Chaves S. Coccygodynia: a proposal for an algorithm for treatment. The Journal of Pain. 2003 Jun 1;4(5):257-66. Link
14. Basson MD. Constipation. Medscape. March 2020. Accessed on June 3, 2022, from: Link
15. Pennekamp PH, Kraft CN, Stütz A, Wallny T, Schmitt O, Diedrich O. Coccygectomy for coccygodynia: does pathogenesis matter?. Journal of Trauma and Acute Care Surgery. 2005 Dec 1;59(6):1414-9. Link
16. Mabrouk A, Alloush A, Foye P. Coccyx Pain. [Updated 2022 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Link
17. Foye PM. Coccydynia: tailbone pain. Physical Medicine and Rehabilitation Clinics. 2017 Aug 1;28(3):539-49. Link
18. Patijn J, Janssen M, Hayek S, Mekhail N, Van Zundert J, Van Kleef M. 14. Coccygodynia. Pain Practice. 2010 Nov;10(6):554-9. Link
19. Lehman JJ. Personal phone discussions and subsequent email correspondence with Tim Bertelsman regarding “coccydynia” on May 28-30, 2022.
20. Patel R, Appannagari A, Whang PG. Coccydynia. Current reviews in musculoskeletal medicine. 2008 Dec;1(3):223-6.
21. Kerr EE, Benson D, Schrot RJ. Coccygectomy for chronic refractory coccygodynia: clinical case series and literature review. Journal of Neurosurgery: Spine. 2011 May 1;14(5):654-63. Link
22. Sandrasegaram N, Gupta R, Baloch M. Diagnosis and management of sacrococcygeal pain. BJA education. 2020 Mar;20(3):74. Link
23. Foye PM. Coccyx Pain Clinical Presentation. Medscape. Retrieved from: Link
24. Nathan ST, Fisher BE, Roberts CS. Coccydynia: a review of pathoanatomy, aetiology, treatment and outcome. The Journal of bone and joint surgery. British volume. 2010 Dec;92(12):1622-7. Link
25. Maigne JY, Chatellier G, Le Faou M, Archambeau M. The treatment of chronic coccydynia with intrarectal manipulation: a randomized controlled study. Spine. 2006 Aug 15;31(18):E621-7. Link
26. Foye PM. Coccydynia: tailbone pain. Physical Medicine and Rehabilitation Clinics. 2017 Aug 1;28(3):539-49. Link
27. Ombregt L, Bisschop P, ter Veer JH. A System of Orthopaedic Medicine. Elsevier Science Limited, 2003, p.968-969.
28. Grieve GP, Pannekoek-Westenburg SJ, Stibbe PD. De wervelkolom: veel voorkomende aandoeningen. De Tijdstroom; 1984.
29. Lehman JJ. Coccygodynia: A pain in the rear. University of Bridgeport Powerpoint presentation.
30. Marinko LN, Pecci M. Clinical decision making for the evaluation and management of coccydynia: 2 case reports. journal of orthopaedic & sports physical therapy. 2014 Aug;44(8):615-21. Link
31. Woon JT, Stringer MD. Clinical anatomy of the coccyx: a systematic review. Clinical anatomy. 2012 Mar;25(2):158-67. Link
32. Thiele GH. Coccygodynia: cause and treatment. Diseases of the Colon & Rectum. 1963 Nov;6(6):422-36. Link
33. Lehman JJ, Morley JJ, Doonan DM. Coccygodynia: A Case Report of Post-Traumatic Pelvic Floor Pain Due to Myofascial Trigger Points. Journal of the American Chiropractic Association. July 2010. Link
34. Skalski MR, Matcuk GR, Patel DB, Tomasian A, White EA, Gross JS. Imaging coccygeal trauma and coccydynia. Radiographics. 2020 Jul;40(4):1090-106. Link
35. Pennekamp PH, Kraft CN, Stütz A, Wallny T, Schmitt O, Diedrich O. Coccygectomy for coccygodynia: does pathogenesis matter?. Journal of Trauma and Acute Care Surgery. 2005 Dec 1;59(6):1414-9. Link
36. Postacchini FR, Massobrio MA. Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. The Journal of bone and joint surgery. American volume. 1983 Oct 1;65(8):1116-24. Link
37. Marinko LN, Pecci M. Clinical decision making for the evaluation and management of coccydynia: 2 case reports. journal of orthopaedic & sports physical therapy. 2014 Aug;44(8):615-21. Link
38. Trollegaard AM, Aarby NS, Hellberg S. Coccygectomy: an effective treatment option for chronic coccydynia: retrospective results in 41 consecutive patients. The Journal of Bone and Joint Surgery. British volume. 2010 Feb;92(2):242-5. Link
39. Capar B, Akpinar N, Kutluay E, Müjde S, Turan A. Coccygectomy in patients with coccydynia. Acta Orthop Traumatol Turc. 2007 Aug 1;41(4):277-80. Link
40. Sandrasegaram N, Gupta R, Baloch M. Diagnosis and management of sacrococcygeal pain. BJA education. 2020 Mar;20(3):74. Link
41. Fogel GR, Cunningham III PY, Esses SI. Coccygodynia: evaluation and management. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2004 Jan 1;12(1):49-54. Link
42. Tuerlinckx M. Physiopedia. Coccydynia, Retrieved from: Link
43. Bergmann TF, Peterson LD, Lawrence DJ. Chiropractic technique: principles and procedures. New York: Churchill Livingstone, 3rd Edition. Chapter 5 - Pelvic Joints, p 274.
44. Polkinghorn BS, Colloca CJ. Chiropractic treatment of coccygodynia via instrumental adjusting procedures using activator methods chiropractic technique. Journal of manipulative and physiological therapeutics. 1999 Jul 1;22(6):411-6. Link
45. Plaugher G, editor. Textbook of clinical chiropractic: a specific biomechanical approach. Williams & Wilkins; 1993.
46. Mohanty PP, Pattnaik M. Effect of stretching of piriformis and iliopsoas in coccydynia. Journal of bodywork and movement therapies. 2017 Jul 1;21(3):743-6. Link
47. Seker A, Sarikaya IA, Korkmaz O, Yalcin S, Malkoc M, Bulbul AM. Management of persistent coccydynia with transrectal manipulation: results of a combined procedure. European Spine Journal. 2018 May;27(5):1166-71. Link
48. Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM&R. 2017 Apr 1;9(4):367-76. Link
49. Maigne JY, Chatellier G. Comparison of three manual coccydynia treatments: a pilot study. Spine. 2001 Oct 15;26(20):E479-83. Link
50. Garg B, Ahuja K. Coccydynia-A comprehensive review on etiology, radiological features and management options. Journal of Clinical Orthopaedics and Trauma. 2021 Jan 1;12(1):123-9. Link
51. Mennel J.B. vol. III. Churchill; 1952. (The Science and Art of Joint Manipulation).
52. Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM&R. 2017 Apr 1;9(4):367-76. Link
53. Coccyx.org. Exercises and yoga for coccyx pain. Retrieved from: Link
54. Mohanty PP, Pattnaik M. Effect of stretching of piriformis and iliopsoas in coccydynia. Journal of bodywork and movement therapies. 2017 Jul 1;21(3):743-6. Link
55. Garg B, Ahuja K. Coccydynia-A comprehensive review on etiology, radiological features and management options. Journal of Clinical Orthopaedics and Trauma. 2021 Jan 1;12(1):123-9. Link
56. Origo D, Tarantino AG, Nonis A, Vismara L. Osteopathic manipulative treatment in chronic coccydynia: a case series. Journal of bodywork and movement therapies. 2018 Apr 1;22(2):261-5. Link
57. Marinko LN, Pecci M. Clinical decision making for the evaluation and management of coccydynia: 2 case reports. journal of orthopaedic & sports physical therapy. 2014 Aug;44(8):615-21. Link
58. Sandrasegaram N, Gupta R, Baloch M. Diagnosis and management of sacrococcygeal pain. BJA education. 2020 Mar;20(3):74. Link
59. Howard PD, Dolan AN, Falco AN, Holland BM, Wilkinson CF, Zink AM. A comparison of conservative interventions and their effectiveness for coccydynia: a systematic review. Journal of Manual & Manipulative Therapy. 2013 Nov 1;21(4):213-9. Link
60. Wu CL, Yu KL, Chuang HY, Huang MH, Chen TW, Chen CH. The application of infrared thermography in the assessment of patients with coccygodynia before and after manual therapy combined with diathermy. Journal of manipulative and physiological therapeutics. 2009 May 1;32(4):287-93. Link
61. Chiarioni G, Asteria C, Whitehead WE. Chronic proctalgia and chronic pelvic pain syndromes: new etiologic insights and treatment options. World Journal of Gastroenterology: WJG. 2011 Oct 28;17(40):4447. Link
62. Nathan ST, Fisher BE, Roberts CS. Coccydynia: a review of pathoanatomy, aetiology, treatment and outcome. The Journal of bone and joint surgery. British volume. 2010 Dec;92(12):1622-7. Link
63. Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM&R. 2017 Apr 1;9(4):367-76. Link
64. Datir A, Connell D. CT-guided injection for ganglion impar blockade: a radiological approach to the management of coccydynia. Clinical radiology. 2010 Jan 1;65(1):21-5. Link
65. Chakraborty S. Nonoperative Management of Coccydynia: A Comparative Study Comparing Three Methods. The Spine Journal. 2012 Sep 1;12(9):S69-70. Link
66. Postacchini FR, Massobrio MA. Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. The Journal of bone and joint surgery. American volume. 1983 Oct 1;65(8):1116-24. Link
67. Pennekamp PH, Kraft CN, Stütz A, Wallny T, Schmitt O, Diedrich O. Coccygectomy for coccygodynia: does pathogenesis matter?. Journal of Trauma and Acute Care Surgery. 2005 Dec 1;59(6):1414-9. Link
68.Perkins R, Schofferman J, Reynolds J. Coccygectomy for severe refractory sacrococcygeal joint pain. Clinical Spine Surgery. 2003 Feb 1;16(1):100-3. Link
69. Thiele GH. Coccygodynia: cause and treatment. Diseases of the Colon & Rectum. 1963 Nov;6(6):422-36. Link
70. Tucker J. Coccyx pain and treatment – Part one. The American Chiropractor. March 2015. Accessed online on 06/08/2022 from Link
71. Tucker J. Coccyx pain and treatment – Part two. The American Chiropractor. July 2015. Accessed online on 06/08/2022 from Link
72. Ladenheim CJ, Sherman RP, Sportelli L. Professional Chiropractic Practice: Ethics, Business, Jurisprudence, and Risk Management: Developing Malpractice Prevention Strategies. PracticeMakers Products; 2001. ISBN# 0-9703839-1-6. p. 24.
73. Tucker J. Personal email correspondence with Tim Bertelsman regarding “coccydynia” on 6/10/2022.