
Rotator Cuff Tears: When to MRI & When to Refer
Reading time: 5 minutes
Your new patient presents with a two-month history of atraumatic-onset right shoulder pain. What’s your most likely diagnosis based on the following limited evaluation findings (AKA- please save the snarky “incomplete H&P” comments 😏):
Pain is localized to the superior and anterolateral shoulder.
Overhead activity and side sleeping exacerbate symptoms.
Abduction and internal rotation are uncomfortable and limited, with mild pain-induced weakness.
There are minimal cervical findings and no signs of radiculopathy.
If you guessed rotator cuff impingement or tendinopathy, you’re probably right!
The preceding history is typical for the spectrum of rotator cuff disorders, plus 65-70% of all shoulder pain diagnoses involve the rotator cuff. (1)
For continuity (and since I’m the one narrating this story), let’s assume that we nailed question number one and suspect a rotator cuff tear. But don’t celebrate yet, because there are a few more essential questions to answer.
Is an MRI always necessary for suspected rotator cuff tears?
When do I need to order a shoulder MRI?
Which orthopedic tests best confirm rotator cuff tears?
When is rotator cuff surgery necessary?
Is conservative chiropractic care appropriate for rotator cuff tears?
Your decisions regarding these issues will impact your clinical outcomes, patient satisfaction, and even liability. This blog will review the current data to help you deliver best practices for rotator cuff problems – so let’s dive in.
1. Is an MRI always necessary for suspected rotator cuff tears?
MRI is an appealing assessment for rotator cuff pathology, showing 90-100% sensitivity and similar specificity for partial or full-thickness tears. (2) And adding arthrography provides even greater sensitivity. (3,4)
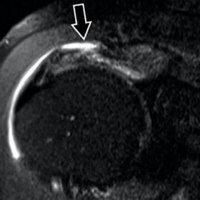
Rotator Cuff Tear: An intermediate signal on T1-weighted images that increases significantly on fluid sensitive sequences (e.g.T2-weighted, STIR, fat saturation, etc.) is indicative of fluid signal, usually within a frank tear, differentiating this from tendinosis/tendinopathy. (5,40)
In many MSK clinics, an MRI is ordered based upon suspicion of almost any rotator cuff pathology. However, research suggests this blanket approach may not be the best practice. The Journal of Shoulder and Elbow Surgery recently concluded (6):
“Over 90% of [rotator cuff] patients had premature MRI. The use of MRI before a trial of conservative management provides negative value in patients with:
atraumatic shoulder pain
minimal to no strength deficits on physical examination
suspected tendinopathy other than full-thickness tears."
2. When do we need to order a shoulder MRI
The primary decision for ordering a shoulder MRI (and most any other diagnostic evaluation) is if the test result will change your subsequent care plan. Some considerations might include:
Significant traumatic onsets
Suspected rotator cuff rupture (i.e., positive drop arm sign) or other significant weakness that is not primarily pain-induced
A failed trial of conservative care
Red flags or suspicion of significant or threatening alternate pathology
Pending referral to a specialist (orthopedist, etc.)
This means most atraumatic chronic shoulder pain patients without significant weakness or suspicion of alternate pathology should undergo a trial of conservative care before advanced imaging.
Pro Tip: The ACR appropriateness criteria® for atraumatic shoulder pain suggest that clinicians might also consider a less costly diagnostic ultrasound evaluation since this test “has been shown to have comparable accuracy to MRI in assessing rotator cuff disease.” (8)
3. Which orthopedic tests best confirm rotator cuff tears
Two simple orthopedic tests have shown excellent ability to help detect rotator cuff tears.

ERLS - External Rotation Lag Sign
“A positive external rotation lag sign is the clinical test most likely to indicate that full-thickness tears of the supraspinatus and infraspinatus are present (specificity, 94%).” (10)
“Pain during DIME testing had a sensitivity of 96.3% and 92.6% in the coronal and scapular planes, respectively…for supraspinatus pathology of any kind (i.e., tendinopathy, “fraying,” or tearing).” (11)

DIME Test
*If you want to learn more about the DIME test, check out this previous blog.
As with any orthopedic assessment, a cluster of tests is more valuable than any isolated maneuver. Two of the more useful additional tests for identifying supraspinatus tears include (12,13):
Jobe / Empty can test (sensitivity 88%, specificity of 62%)
Full can test (sensitivity 70%, specificity of 81%)
Jobe / Empty Can Test

Full Can Test
The Lancet journal previously reported a 98% probability of full-thickness rotator cuff tear when three of the following findings were present (9):
Age over 60
Weakness in resisted external rotation
Supraspinatus weakness (Empty Can Test)
Positive signs of impingement (Neer, Hawkins)
4. When is rotator cuff surgery necessary
“Guidelines for treatment, whether operative or nonoperative, are ambiguous at best.” (14)
Definitive guidelines for surgical rotator cuff repair are lacking, partially because a multitude of factors needs to be considered, including age, gender, the timing of onset, duration of symptoms, range of motion and strength deficits, size of the tear, response to prior care, and overall health status. (13,14)
A synthesis of the literature suggests that a rotator cuff surgical consult may be indicated for (but not limited to) the following situations (13-16):
Tendon ruptures
Large, full-thickness tears (> 1-3 cm)
Functional impairment/ weakness
Failed 6-12 week trial of conservative care
For the remaining majority of chronic, less complex cases, multiple studies have shown no advantage for surgery vs. conservative care for rotator cuff tears. (32-37) One large study summarized the current consensus on uncomplicated tears:
"[Surgery] may provide little or no clinically important benefits with respect to pain, function, overall quality of life or … treatment success when compared with non-operative treatment." (32)
Is your patient considering a steroid shot as a last-ditch effort before surgery?
“A single rotator cuff corticosteroid injection (in the year before surgery) is associated with 1.3- 2.8 times increased risk of needing revision rotator cuff repair.” (17)
5. Is conservative chiropractic care appropriate for rotator cuff tears?
Simple answer: Yes! Conservative care should be the first choice for most rotator cuff tears (16,18-21)
“Non-surgical management is always appropriate, providing [patients] are responding with improved function and decreased pain.” (16)
Non-surgical management of partial-thickness and chronic full-thickness tears yields good outcomes (29-31) that rival or surpass surgical results. (21-23)
Plus, our primary tool, spinal manipulation, has been shown to decrease shoulder pain while improving mobility and function. (24-28,38)
“Active shoulder flexion and abduction mobility increase after manipulation of thoracic spine in (rotator cuff) patients. Subacromial space increases significantly after manipulation.” (38)
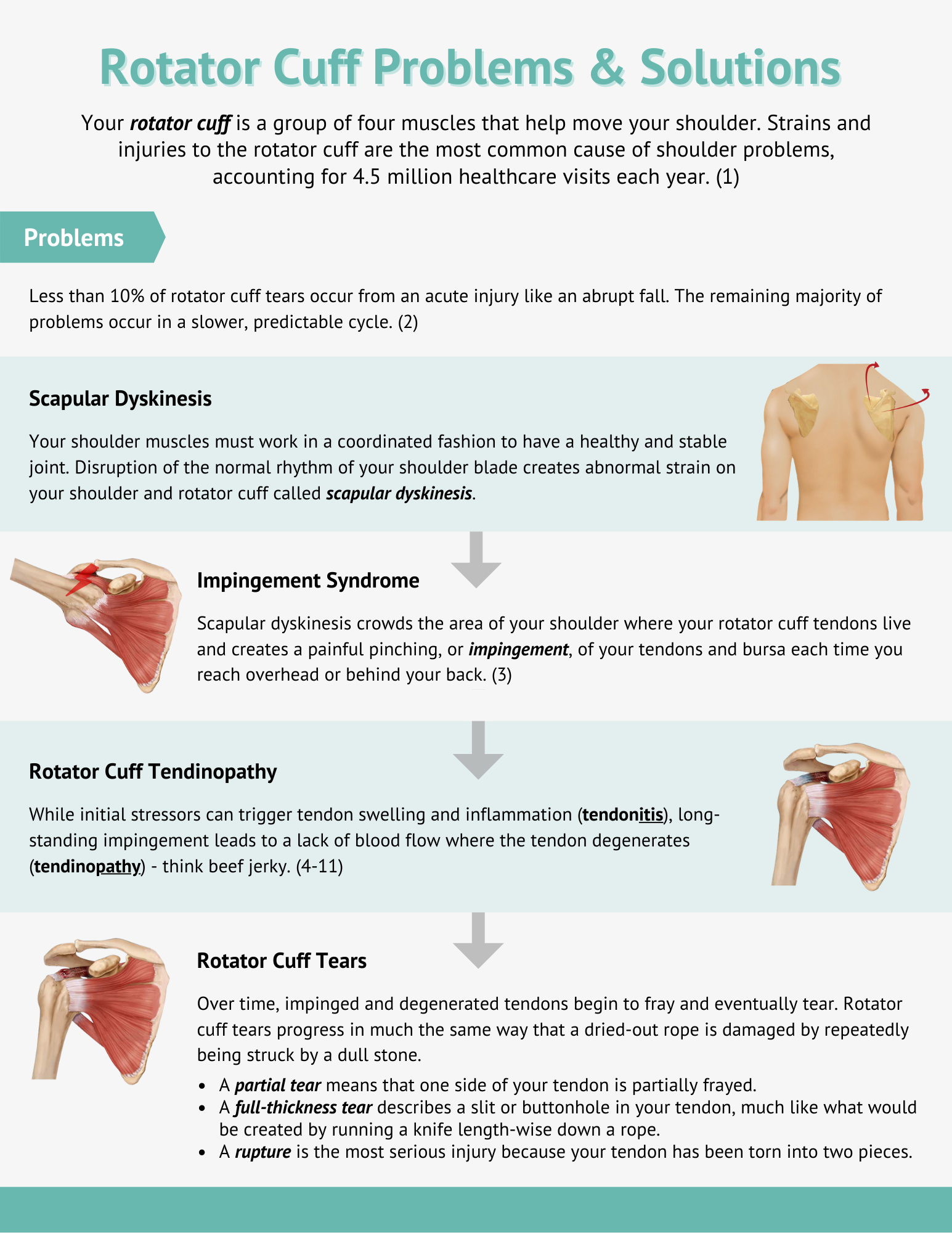
Pro Tip: Use this Rotator Cuff Problems & Solutions infographic to educate your patients and social media followers about how chiropractic care can help resolve rotator cuff problems.
Data suggests that 6-12 weeks is a reasonable conservative care timeframe for most patients before considering surgery. (39) But there’s a vast difference between merely treating someone and consistently applying best practices. And ChiroUp helps you deliver the latter!
Want to gain new skills and greater confidence to resolve shoulder complaints, regardless of the diagnosis? Then check out our latest webinar!

-
1. Jain NB, Fan R, Higgins LD, Kuhn JE, Ayers GD. Does my patient with shoulder pain have a rotator cuff tear? A predictive model from the ROW cohort. Orthopaedic Journal of Sports Medicine. 2018 Jul 16;6(7):2325967118784897. Link
2. Sharma G, Bhandary S, Khandige G, Kabra U. MR imaging of rotator cuff tears: correlation with arthroscopy. Journal of clinical and diagnostic research: JCDR. 2017 May;11(5):TC24. Link
3. Small KM, Adler RS, Shah SH, Roberts CC, Bencardino JT, Appel M, Gyftopoulos S, Metter DF, Mintz DN, Morrison WB, Subhas N. ACR Appropriateness Criteria® shoulder pain-atraumatic. Journal of the American College of Radiology. 2018 Nov 1;15(11):S388-402. Link
4. Huang T, Liu J, Ma Y, Zhou D, Chen L, Liu F. Diagnostic accuracy of MRA and MRI for the bursal-sided partial-thickness rotator cuff tears: a meta-analysis. Journal of orthopaedic surgery and research. 2019 Dec;14(1):1-1. Link
5. Malanga G. (2018). Rotator Cuff Injury Workup. Retrieved from Medscape: https://emedicine.medscape.com/article/92814-workup
6. Cortes A, Quinlan NJ, Nazal MR, Upadhyaya S, Alpaugh K, Martin SD. A value-based care analysis of magnetic resonance imaging in patients with suspected rotator cuff tendinopathy and the implicated role of conservative management. Journal of Shoulder and Elbow Surgery. 2019 Nov 1;28(11):2153-60. Link
7. Intentionally blank
8. Small KM, Adler RS, Shah SH, Roberts CC, Bencardino JT, Appel M, Gyftopoulos S, Metter DF, Mintz DN, Morrison WB, Subhas N. ACR Appropriateness Criteria® shoulder pain-atraumatic. Journal of the American College of Radiology. 2018 Nov 1;15(11):S388-402. Link
9. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. The Lancet. 2001 Mar 10;357(9258):769-70. Link
10. Miller CA, Forrester GA, Lewis JS. The validity of the lag signs in diagnosing full-thickness tears of the rotator cuff: a preliminary investigation. Archives of physical medicine and rehabilitation. 2008 Jun 1;89(6):1162-8. Link
11. Abraham PF, Nazal MR, Varady NH, Gillinov SM, Quinlan NJ, Alpaugh K, Martin SD. The new dynamic isotonic manipulation examination (DIME) is a highly sensitive secondary screening tool for supraspinatus full-thickness tears. Journal of Shoulder and Elbow Surgery. 2020 Nov 1;29(11):2213-20. Link
12. Jain NB, Luz J, Higgins LD, Dong Y, Warner JJ, Matzkin E, Katz JN. The diagnostic accuracy of special tests for rotator cuff tear: the ROW cohort study. American journal of physical medicine & rehabilitation. 2017 Mar;96(3):176. Link
13. Weber S, Chahal J. Management of rotator cuff injuries. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2020 Mar 1;28(5):e193-201. Link
14. Oh LS, Wolf BR, Hall MP, Levy BA, Marx RG. Indications for rotator cuff repair: a systematic review. Clinical Orthopaedics and Related Research®. 2007 Feb 1;455:52-63. Link
15. Bartolozzi A, Andreychik D, Ahmad S. Determinants of outcome in the treatment of rotator cuff disease. Clinical orthopaedics and related research. 1994 Nov 1(308):90-7. Link
16. May T, Garmel GM. Rotator cuff injury. Link
17. Puzzitiello RN, Patel BH, Nwachukwu BU, Allen AA, Forsythe B, Salzler MJ. Adverse impact of corticosteroid injection on rotator cuff tendon health and repair: a systematic review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2020 May 1;36(5):1468-75. Link
18. Longo UG, Franceschi F, Berton A, Maffulli N, Droena V. Conservative treatment and rotator cuff tear progression. Rotator Cuff Tear. 2012;57:90-9. Link
19. Kukkonen J, Joukainen A, Lehtinen J, Mattila KT, Tuominen EK, Kauko T, Äärimaa V. Treatment of non-traumatic rotator cuff tears: A randomised controlled trial with one-year clinical results. The bone & joint journal. 2014 Jan;96(1):75-81. Link
20. Edwards P, Ebert J, Joss B, Bhabra G, Ackland T, Wang A. Exercise rehabilitation in the non-operative management of rotator cuff tears: a review of the literature. International journal of sports physical therapy. 2016 Apr;11(2):279. Link
21. Lewis J. Rotator cuff related shoulder pain: assessment, management and uncertainties. Manual therapy. 2016 Jun 1;23:57-68. Link
22. Boorman RS, More KD, Hollinshead RM, Wiley JP, Mohtadi NG, Lo IK, Brett KR. What happens to patients when we do not repair their cuff tears? Five-year rotator cuff quality-of-life index outcomes following nonoperative treatment of patients with full-thickness rotator cuff tears. Journal of shoulder and elbow surgery. 2018 Mar 1;27(3):444-8. Link
23. Challoumas D, Clifford C, Kirwan P, Millar NL. How does surgery compare to sham surgery or physiotherapy as a treatment for tendinopathy? A systematic review of randomised trials. BMJ open sport & exercise medicine. 2019 Apr 1;5(1):e000528. Link
24. Crosbie J, Kilbreath SL, Hollmann L, York S. Scapulohumeral rhythm and associated spinal motion. Clinical biomechanics. 2008 Feb 1;23(2):184-92. Link
25. Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. Journal of Manual & Manipulative Therapy. 2009 Dec 1;17(4):230-6. Link
26. Walser RF, Meserve BB, Boucher TR. The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials. Journal of Manual & Manipulative Therapy. 2009 Dec 1;17(4):237-46. Link
27. Khan K, Cook J. The painful nonruptured tendon: clinical aspects. Clinics in sports medicine. 2003 Oct 1;22(4):711-25. Link
28. Southerst D, Yu H, Randhawa K, Côté P, D’Angelo K, Shearer HM, Wong JJ, Sutton D, Varatharajan S, Goldgrub R, Dion S. The effectiveness of manual therapy for the management of musculoskeletal disorders of the upper and lower extremities: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Chiropractic & manual therapies. 2015 Dec;23(1):30. Link
29. Tashjian RZ. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clinics in sports medicine. 2012 Oct 1;31(4):589-604. Link
30. Ainsworth R, Lewis JS. Exercise therapy for the conservative management of full thickness tears of the rotator cuff: a systematic review. British journal of sports medicine. 2007 Apr 1;41(4):200-10. Link
31. Baydar M, Akalin E, El O, Gulbahar S, Bircan C, Akgul O, Manisali M, Orhan BT, Kizil R. The efficacy of conservative treatment in patients with full-thickness rotator cuff tears. Rheumatology international. 2009 Apr 1;29(6):623-8. Link
32. Karjalainen TV, Jain NB, Heikkinen J, Johnston RV, Page CM, Buchbinder R. Surgery for rotator cuff tears. Cochrane Database of Systematic Reviews. 2019(12). Link
33. Ranebo MC, Hallgren HC, Holmgren T, Adolfsson LE. Surgery and physiotherapy were both successful in the treatment of small, acute, traumatic rotator cuff tears: a prospective randomized trial. Journal of shoulder and elbow surgery. 2020 Mar 1;29(3):459-70. Link
34. Cederqvist S, Flinkkilä T, Sormaala M, Ylinen J, Kautiainen H, Irmola T, Lehtokangas H, Liukkonen J, Pamilo K, Ridanpää T, Sirniö K. Non-surgical and surgical treatments for rotator cuff disease: a pragmatic randomised clinical trial with 2-year follow-up after initial rehabilitation. Annals of the Rheumatic Diseases. 2020 Dec 3. Link
35. Karasuyama M, Gotoh M, Tahara K, Kawakami J, Madokoro K, Nagamatsu T, Imai T, Harada N, Kudo Y, Shiba N. Clinical results of conservative management in patients with full-thickness rotator cuff tear: a meta-analysis. Clinics in Shoulder and Elbow. 2020 Jun;23(2):86. Link
36. Kozono N, Takeuchi N, Okada T, Hamai S, Higaki H, Shimoto T, Ikebe S, Gondo H, Senju T, Nakashima Y. Dynamic scapulohumeral rhythm: Comparison between healthy shoulders and those with large or massive rotator cuff tear. Journal of Orthopaedic Surgery. 2020 Dec 22;28(3):2309499020981779. Link
37. Kukkonen J, Ryösä A, Joukainen A, Lehtinen J, Kauko T, Mattila K, Äärimaa V. Operative Vs. Conservative Treatment Of Small Non-Traumatic Supraspinatus Tears In Patients Over 55 Years: Over 5-Year Follow-Up Of A Randomized Controlled Trial. Journal of Shoulder and Elbow Surgery. 2021 Mar 24. Link
38. Belón-Perez, Pedro et al. Immediate Effects of Thoracic Spine Manipulation Upon Shoulder Functionality in Patients With Sutured Rotator Cuff Repair: A Prospective Study Journal of Manipulative & Physiological Therapeutics , Volume 41 , Issue 7 , 589 – 595. Link
39. Schmidt CC, Jarrett CD, Brown BT. Management of rotator cuff tears. The Journal of hand surgery. 2015 Feb 1;40(2):399-408. Link
40. MRI Imaging. Personal email from Michael Barry DACBR to Tim Bertelsman on 05/04/2022 regarding MRI imaging for rotator cuff pathology.