
Conservative Treatments for Knee Osteoarthritis: Evidence-Based Options for Chiropractors

Knee osteoarthritis is one of the leading causes of pain and disability in adults over 60. Up to 16% of the population experiences the condition’s hallmark pain, stiffness, and functional limitation, often leading to reduced mobility, diminished quality of life, and escalating healthcare costs from medications and joint replacement surgeries. (1)
For decades, the default response for knee osteoarthritis treatment has been medication — most often NSAIDs and acetaminophen. While these drugs provide temporary relief, they come with well-known risks: gastrointestinal bleeding, cardiovascular events, and even increased mortality in older patients with comorbidities. (24,25)
The good news? Research confirms that conservative, non-drug therapies often rival or outperform medications for knee osteoarthritis pain relief — without the dangerous side effects. (2-4,19,23,24) Many chiropractors are uniquely positioned to deliver these therapies, combining manual expertise, functional rehabilitation, and evidence-based adjunctive tools.*
This blog reviews the evidence supporting the conservative tools many chiropractors use daily plus the ranked adjunctive modalities from a 2025 network meta-analysis that evaluated 139 randomized controlled trials. (2) Together, these insights strengthen chiropractic’s role at the forefront of musculoskeletal care.
Practical, Evidence-Supported Tools for Knee Osteoarthritis
Chiropractors already have a powerful toolbox for managing knee osteoarthritis, and the research increasingly supports what we do daily. From joint and soft-tissue interventions to needling, nutrition, and patient education, these strategies improve pain, mobility, and quality of life. Here are some of the most effective approaches.
Joint Manipulation / Mobilization for Knee Osteoarthritis
Gentle oscillatory mobilization and axial distraction restore joint mechanics, improve synovial fluid distribution, and reduce nociceptive input. Adding manual therapy, including joint manipulation/ mobilization, to rehabilitation programs enhances outcomes with pain reduction and functional gains. (4-10)


ChiroUp Essentials subscribers can access the full tutorial videos for each of these skills (and hundreds more) through their Clinical Skills tab. ChiroUp EHR subscribers can pull them up directly within their SOAP notes, putting real-world tools at their fingertips and helping them become better clinicians with every visit.
Nerve Mobilization for Knee Osteoarthritis
Emerging evidence suggests that neurodynamic techniques, such as nerve flossing and nerve release, may help reduce pain and improve function in knee osteoarthritis by mobilizing the nerves that transmit nociceptive input from the joint. (26) The most relevant targets include the saphenous/ femoral, tibial, obturator, and common peroneal nerves, which collectively supply the anterior, medial, posterior, and lateral knee capsule.



Check out our prior Lower Extremity Neurodynamics blog for details.
Myofascial Release for Knee Osteoarthritis
Myofascial release reduces abnormal muscle tension, improves mobility, and restores gait mechanics by addressing periarticular and hip restrictions. Targeted release of the TFL, hamstrings, quads, gastroc, and adductors is especially impactful for pain reduction and functional restoration. (4,11)



Instrument-Assisted Soft Tissue Mobilization (IASTM) for Knee Osteoarthritis
IASTM helps disrupt pericapsular adhesions, improves tissue glide, and enhances functional ROM. It is particularly useful for addressing chronic stiffness and can amplify exercise outcomes. (12,13)

Acupuncture for Knee Osteoarthritis
Acupuncture stimulates opioid-mediated descending pain pathways and modulates inflammation. Although evidence is mixed, several trials demonstrate pain and function improvements when acupuncture is integrated into a comprehensive plan of care. (14-17)
Dry Needling for Knee Osteoarthritis
By disrupting dysfunctional motor end plates in quadriceps and gastrocnemius trigger points, dry needling reduces nociceptive input, decreases central sensitization, and restores muscle activation. Clinical trials report short-term pain relief, with one study showing greater benefit than oral diclofenac. (18,19)
Glucosamine & Chondroitin for Knee Osteoarthritis
Nutritional support with glucosamine sulfate (often paired with chondroitin) may help support cartilage metabolism and reduce inflammation. While results vary, some studies show superior outcomes when supplementation is combined with exercise. (20-23)
Education
One of our most potent tools is counseling and education (4) — empowering patients to help themselves through various avenues.
Selecting osteoarthritis knee exercises
Activity pacing
Posture, Ergonomics, & Biomechanics
Walking aids (eg, canes)
Orthotics and footwear
Hydration & nutrition
Weight management
Chronic pain–coping strategies
Sleep hygiene
Use of topical creams for symptomatic relief
Delivering all of this education is one of the most valuable things we do for patients, but it can also be time-consuming and easy to overlook details in the moment. Fortunately, ChiroUp subscribers can provide comprehensive education in just four clicks. Check out this quick demo to see how it works.
And if you’re already using our Essentials platform, have you explored the new ChiroUp EHR? It blends all your favorite features into your daily workflow, making your job even easier.
2025 Systematic Review: Ranked Adjunctive Knee Osteoarthritis Treatments
In June 2025, Chen et al. published a landmark network meta-analysis evaluating 12 modalities for OA knee treatment across 139 randomized controlled trials. (2) Importantly, this analysis did not include many of the previously mentioned hands-on and nutritional tools chiropractors use. Still, it does provide a comparative effectiveness ranking of additional knee osteoarthritis treatment strategies that may enhance care.
Most Effective Options
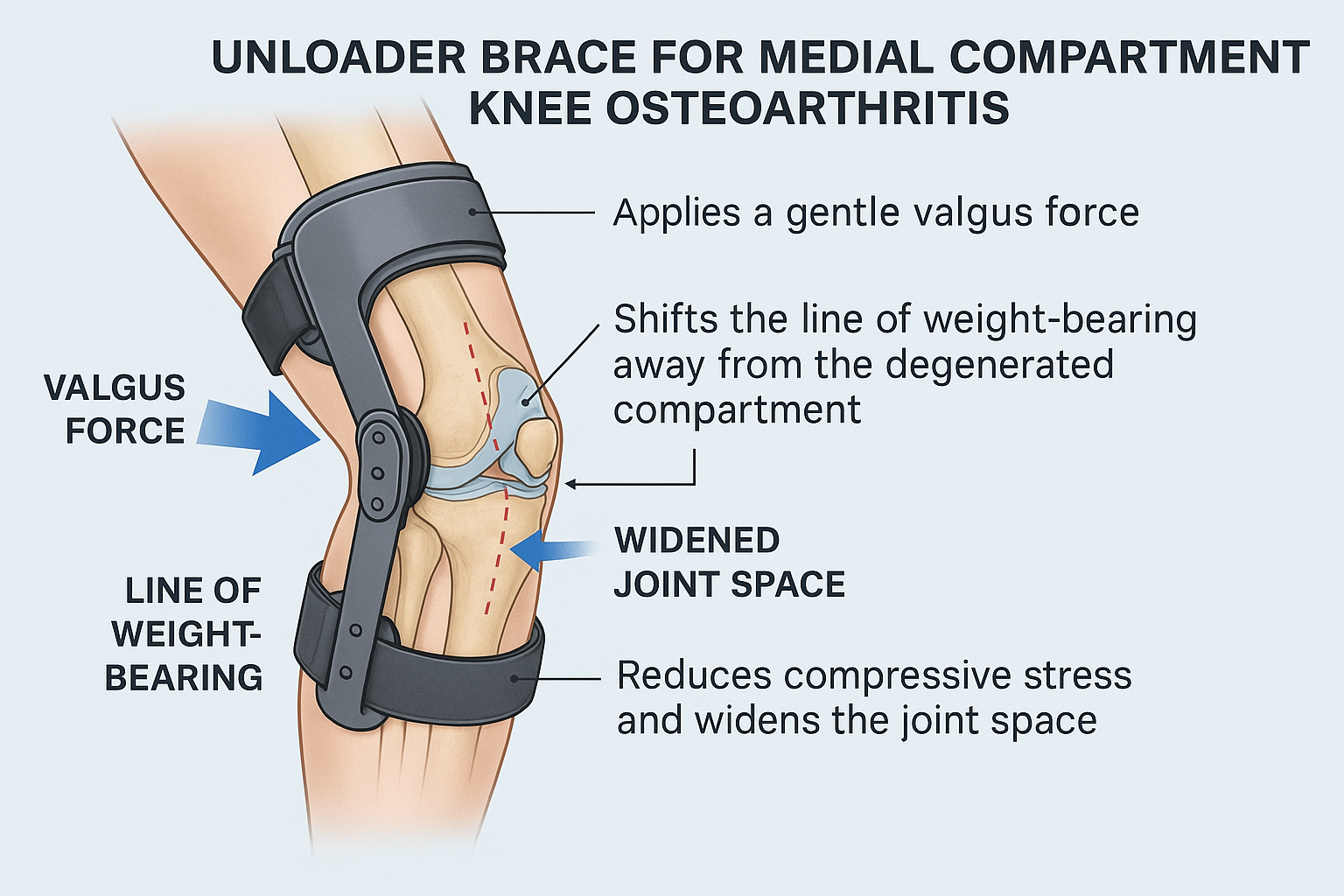
1. Osteoarthritis Knee Braces
An unloader brace for knee osteoarthritis is a simple but powerful tool for patients with medial compartment knee osteoarthritis. By applying a gentle valgus force, these braces shift the line of weight-bearing away from the degenerated compartment, reducing compressive stress and widening the joint space during gait. Clinically, this translates into less pain, improved walking mechanics, and greater functional tolerance for daily activities. Beyond offloading cartilage, knee unloader braces also enhance proprioception, stabilize the knee in unstable conditions, and reduce muscle fatigue—all of which help prolong mobility and delay disease progression. The result is immediate gait improvement and pain relief, making a knee support for osteoarthritis one of the most effective non-drug treatments.
2. Hydrotherapy (Aquatic Exercise for Knee Joint Osteoarthritis)
Exercising in warm water reduces joint load while providing resistance for circulation, relaxation, and strength. Hydrotherapy exercises for knee osteoarthritis significantly reduce pain and improve function, particularly for patients who cannot tolerate land-based exercise.
3. Exercises for Knee Osteoarthritis
Knee OA exercises remain a foundational tool. Aerobic and mind-body activities (such as yoga) show the most substantial benefits, while strengthening and flexibility programs also improve pain and function. Knee exercises for osteoarthritis are indispensable for long-term outcomes. However, providers must also address the associated kinetic chain functional deficits that perpetuate knee pain.
Want a deeper dive? Check out ChiroUp’s free webinars on two of the most common biomechanical deficits—hip abductor weakness and foot hyperpronation. Each session gives you a complete rundown and practical skills you can put to work immediately to address factors that perpetuate knee pain.
Moderately Effective Options
4. High-Intensity Laser Therapy (HILT)
Penetrates deeply to deliver strong anti-inflammatory and analgesic effects. Outperforms Low-Level Laser Therapy for knee osteoarthritis and provides substantial symptom reduction.
5. Extracorporeal Shockwave Therapy (ESWT)
Applies acoustic waves to stimulate circulation and tissue repair. Effective in reducing pain and improving function, especially when conventional progress plateaus.
6. Low-Level Laser Therapy (LLLT)
Stimulates cellular metabolism, reduces inflammation, and promotes repair. Less potent than High Level Laser Therapy for knee osteoarthritis, but still an effective adjunct.


Supportive Options
7. Transcutaneous Electrical Nerve Stimulation (TENS)
Blocks pain signals through neural modulation, providing short-term relief as a supportive therapy.
8. Interferential Current (IFC)
Medium-frequency electrical stimulation penetrates deeper than TENS. Offers modest pain and circulation benefits.
9. Elastic Therapeutic taping/ Kinesio Taping (KT)
Supports motion, enhances proprioception, and may reduce pain temporarily.
This review by Chen et al. (2) also evaluated shortwave diathermy, ultrasound therapy, and lateral wedge insoles for knee osteoarthritis treatment. Each of these modalities demonstrated some short-term benefit but offered limited or questionable long-term effectiveness compared to higher-ranked modalities.
Why This Matters for Chiropractors
The data is clear: simple conservative therapies frequently outperform medications for knee OA pain relief. Chiropractors deliver many of these effective knee osteoarthritis treatments daily and are positioned as primary providers for patients seeking safe, effective alternatives to drugs and injections.
At the same time, best practice often involves co-management, with medications playing a supportive role when needed. And some patients will ultimately require surgical intervention. Recognizing where each tool fits only strengthens chiropractic’s role in the broader healthcare system.
This research reinforces chiropractic’s value. To help spread this message, we’ve created a new knee osteoarthritis treatment infographic that ChiroUp subscribers can share with patients and social media followers.* It’s a simple, eye-opening way to show how evidence-based conservative care can reduce pain, restore mobility, and improve lives.

Conclusion
Knee osteoarthritis is a common, disabling condition, but it doesn’t require a lifetime of medication dependence. Research shows that chiropractic tools like manipulation, soft-tissue therapies, acupuncture, dry needling, and supplementation effectively reduce pain and improve function. Meanwhile, the Chen et al. systematic review highlights additional adjunctive modalities that can further enhance outcomes when integrated appropriately.
Bottom line: Conservative therapies aren’t just safer — they’re often more effective than medications. Chiropractors are ideally positioned to lead the way in delivering these evidence-based solutions.
At ChiroUp, we give you the tools to lead with confidence, elevate your patient outcomes, and stay ahead of the curve in a profession that is evolving every day.
Let’s take the next step together. Schedule a demo with our team to share your clinic’s unique needs and pain points, and see how ChiroUp’s solutions can become the partner you’ve been missing.
-
1. Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020 Dec 1;29. Link
2. Chen X, Fan Y, Tu H, Luo Y. Clinical efficacy of different therapeutic options for knee osteoarthritis: A network meta-analysis based on randomized clinical trials. PLoS One. 2025 Jun 18;20(6):e0324864. Link3. Simple therapies outperform drugs for knee arthritis pain relief. ScienceDaily [Internet]. 20 Sep 2025 [cited 2025 Sep 21]. Available from: Link
4. Zhang W, Moskowitz R, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis and Cartilage. 2008;16:137-162. Link
5. Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD, Hutton JP, Henderson NE, Garber MB. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Physical therapy. 2005 Dec 1;85(12):1301-17. Link
6. Brantingham JW, Globe G, Pollard H, Hicks M, Korporaal C, Hoskins W. Manipulative therapy for lower extremity conditions: expansion of literature review. Journal of manipulative and physiological therapeutics. 2009 Jan 1;32(1):53-71. Link
7. Hoeksma HL, Dekker J, Ronday HK, Heering A, Van Der Lubbe N, Vel C, Breedveld FC, Van Den Ende CH. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial. Arthritis Care & Research: Official Journal of the American College of Rheumatology. 2004 Oct 15;51(5):722-9. Link
8. Pollard H, Ward G, Hoskins W, Hardy K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: a randomised controlled trial. The Journal of the Canadian Chiropractic Association. 2008 Dec;52(4):229. Link
9. Tucker ML. The relative effectiveness of a non-steroidal anti-inflammatory medication (meloxicam) versus manipulation in the treatment of osteoarthritis of the knee (Doctoral dissertation). Link
10. Dwyer L, Parkin-Smith GF, Brantingham JW, Korporaal C, Cassa TK, Globe G, Bonnefin D, Tong V. Manual and manipulative therapy in addition to rehabilitation for osteoarthritis of the knee: assessor-blind randomized pilot trial. Journal of manipulative and physiological therapeutics. 2015 Jan 1;38(1):1-21. Link
11. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Archives of Internal Medicine. 2006 Dec 11;166(22):2533-8. Link
12. Karimi Soloklo, Z., Boozari, S. and Kahrizi, S., 2025. Effects of a two-week instrument-assisted soft tissue mobilization and exercise therapy versus sham and exercise on gait kinetics in moderate knee osteoarthritis: a randomized controlled trial. Journal of Manual & Manipulative Therapy, pp.1-12 Link
13. Anjum, N., Sheikh, R.K., Omer, A., Anwar, K., Khan, M.M.H., Aftab, A. and Awan, W.A., 2023. Comparison of instrument-assisted soft tissue mobilization and proprioceptive neuromuscular stretching on hamstring flexibility in patients with knee osteoarthritis. PeerJ, 11, p.e16506. Link
14. Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee. Ann Intern Med. 2004 Dec 1;141(12):901-10. Link
15. Lin X, Huang K, Zhu G, Huang Z, Qin A, Fan S. The effects of acupuncture on chronic knee pain due to osteoarthritis: a meta-analysis. JBJS. 2016 Sep 21;98(18):1578-85. Link
16. Zhang Y, Wang C. Acupuncture and Chronic Musculoskeletal Pain. Current Rheumatology Reports. 2020 Nov;22(11):1-1. Link
17. Lin X, Li F, Lu H, Zhu M, Peng TZ. Acupuncturing of myofascial pain trigger points for the treatment of knee osteoarthritis: A systematic review and meta-analysis. Medicine. 2022 Feb 25;101(8). Link
18. Amani M, Shafizadegan Z, Taheri N. Effects of dry needling on pain in patients with knee osteoarthritis: A preliminary study. Advanced Biomedical Research. 2022;11. Link
19. Ma YT, Dong YL, Wang B, Xie WP, Huang QM, Zheng YJ. Dry needling on latent and active myofascial trigger points versus oral diclofenac in patients with knee osteoarthritis: a randomized controlled trial. BMC Musculoskeletal Disorders. 2023 Dec;24(1):1-3. Link
20. Richy F, Bruyere O, Ethgen O, Cucherat M, Henrotin Y, Reginster JY. Structural and symptomatic efficacy of glucosamine and chondroitin in knee osteoarthritis: a comprehensive meta-analysis. Archives of Internal Medicine. 2003 Jul 14;163(13):1514-22. Link
21. Vo NX, Le NN, Chu TD, Pham HL, Dinh KX, Che UT, Ngo TT, Bui TT. Effectiveness and safety of glucosamine in osteoarthritis: a systematic review. Pharmacy. 2023 Aug;11(4):117. Link
22. Meng Z, Liu J, Zhou N. Efficacy and safety of the combination of glucosamine and chondroitin for knee osteoarthritis: a systematic review and meta-analysis. Archives of orthopaedic and trauma surgery. 2023 Jan;143(1):409-21. Link
23. Hochberg MC, Martel-Pelletier J, Monfort J, Möller I, Castillo JR, Arden NK, Berenbaum F, Blanco-García FJ, Conaghan PG, Domènech Carbó G, Henrotin Y. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis. Link
24. Weng, Q., Goh, S.L., Wu, J., Persson, M.S., Wei, J., Sarmanova, A., Li, X., Hall, M., Doherty, M., Jiang, T. and Zeng, C., 2023. Comparative efficacy of exercise therapy and oral non-steroidal anti-inflammatory drugs and paracetamol for knee or hip osteoarthritis: a network meta-analysis of randomised controlled trials. British journal of sports medicine, 57(15), pp.990-996. Link
25. Zeng C, Zhang W, Doherty M, Persson MS, Mallen C, Swain S, Li X, Wei J, Lei G, Zhang Y. Initial analgesic prescriptions for osteoarthritis in the United Kingdom, 2000–2016. Rheumatology. 2021 Jan;60(1):147-59. Link
26. Serrano-García B, Martínez-Cepa CB, Forriol F, Zuil-Escobar JC. Active Neurodynamic Technique at Home in Patients with Knee Osteoarthritis: An Open Single Arm Clinical Trial. Medicina. 2024 Nov 12;60(11):1857. Link
*Chiropractors considering therapies such as extremity adjustments, acupuncture, dry needling, nutritional counseling, or therapeutic modalities like laser should always consult their individual state statutes and licensing boards, since the scope of practice varies by jurisdiction. While most of these services are permitted in most states, some require additional certification (e.g., acupuncture or dry needling), and others may be restricted or prohibited in a minority of jurisdictions.