
Cervicogenic Headache: Lasting Benefits of MSK Care
On July 4, 2020, the European Journal of Pain published a study that would pique the interest of most evidence-based chiropractors - Spinal manipulation for the management of cervicogenic headache: a systematic review and meta-analysis. While this review highlighted the utility of SMT, the paper’s conclusion was slightly disparaging:
For cervicogenic headache, SMT provides superior short-term benefits for pain intensity, frequency and disability…The long-term impact is not significant. (25)
“Not significant” ???
For patients, payors, and non-DC healthcare providers, the take-away is not ideal: SMT is a relatively costly analgesic when used in isolation. Not so exciting anymore, huh?
Fortunately, we can change that message. This week’s blog and video will detail three tools that evidence-based chiropractors can employ, in addition to SMT, to provide lasting benefit for cervicogenic headache patients.
Defining Value
The Fernandez study is troubling because it implies that isolated SMT provides little long-term value. As illustrated in the simple formula below, safe, timely, and lasting results are vital metrics when defining value in the current healthcare model.
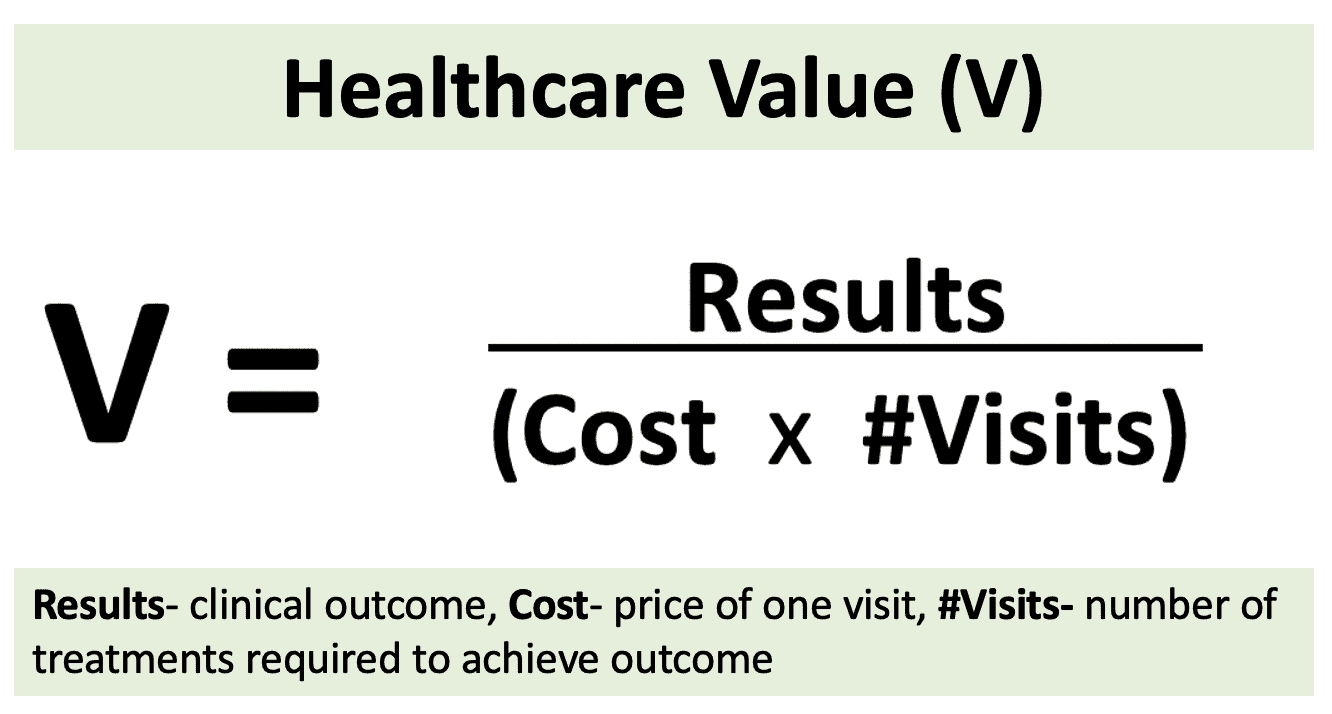
In this simple “value” formula, increasing the numerator improves a provider’s value to patients and payors. Anything that increases the denominator makes the provider less valuable. Fernendez’s (25) conclusion suggests that isolated SMT provides short-term relief of CGH symptoms without lasting benefit. This equates to an undesirable decrease in value.
Centration- The Key to MSK Value
Cervicogenic headaches and many other common MSK problems redevelop when their underlying triggers are not resolved. Those triggers are related to the patient’s activities, postures, and learned patterns of muscular imbalance. Anything that places enough stress on a system will painfully locate the weak link in that system.
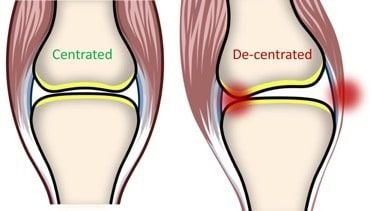
Joint “centration” refers to functional joint alignment, and can be defined as “maintaining optimal surface relationships throughout the range of motion.”
To illustrate, consider the example of flexing and extending your index finger a thousand times. A healthy, “centrated” joint would have little trouble with this task. Now, imagine stretching two identical rubber bands from the tip of that index finger – one pulling medially and the other pulling laterally. Although these bands add load, the balanced arrangement should allow the joint to function in a centrated fashion, without significant sequelae. However, what would happen if one band was significantly thicker or tighter than the other? This imbalance would “de-centrate” the joint, compressing cartilage on one side and stretching contralateral tissues.
In simple terms, chronically compressed joint cartilage leads to a continuum beginning with irritation and transitioning into restricted joints. Isolated SMT addresses the symptom of restriction, but does little to address the underlying “decentrating” causes – meaning the problem will likely return, and painfully, “the long-term impact is not significant.”
Creating lasting value requires consistent identification of muscular imbalances and functional deficits that cause joint dysfunction. Fortunately, evidence-based chiropractors employ a plethora of tools that help centrate joints and achieve long-term results. Check out this recent blog video and tutorial to review three of our top tools for resolving cervicogenic headaches.
The Chief Complaint
Cervicogenic headache (CGH) patients present with neck tenderness and stiffness. By definition, CGH is unilateral without side shift, but in some cases, the condition may present bilaterally. Moderate to severe pain may begin in the cervical spine and progressively affect the occipital, temporal, frontal, or supraorbital regions. In some instances, pain may refer to the ipsilateral arm. (17) Symptomatic episodes may last hours to days. The characteristic continuous, fluctuating pain is described as “deep” but generally not throbbing. Symptoms may be triggered or reproduced by sustained or awkward cervical spine postures. (18)
The Solutions
Most every manual therapist agrees that manipulation is an essential component for managing CGH. However, as mentioned earlier, the successful long-term resolution of CGH patients often requires a multifaceted approach that includes more than isolated SMT. So here are three ancillary tools to help you assess and manage this problem more quickly and completely.
1. Assessment: Deep Neck Flexors
Upper cervical joint dysfunction is a key finding in CGH patients. In many cases, this dysfunction is secondary to chronic muscular imbalance and sustained poor posture. Loss of strength in the deep neck flexors and over-activation of the SCM and upper trapezius is a common finding in CGH patients. (19,20) Janda recommends screening for neck flexor weakness with the Neck Flexion Test. (19)
In this test, the supine patient is asked to lift their head several inches off of the table to look at their toes. The clinician observes for a "normal" movement pattern - initiated with a chin tuck and smooth reversal of the cervical lordosis. An "abnormal" screen would result in the chin moving forward into protraction from overcompensation by the SCM. The normal firing pattern for this movement is longus capitus, longus colli, SCM, and finally, anterior scalenes. Abnormal movement patterns suggest weakness of the deep neck flexors.

The Deep neck flexor endurance test is another valuable tool to screen for weakness. (21,22)
From a supine hook-lying position, the patient performs chin retraction and then lifts their head an inch off the table. The clinician places their flat hand on the table below the patient’s occiput. If the patient’s head begins to lower or their anterior neck skin folds separate, they are reminded to “tuck your chin and hold your head up.” The test is timed until the patient’s head touches the clinician’s hand for more than one second. The average endurance for men is about 40 seconds and 30 for women. Those with neck pain average closer to 20 seconds. Low times suggest neck flexor weakness with a predisposition to over-utilize the SCM, platysma, and hyoid, resulting in a forward head posture and neck pain.
2. Treatment: Nerve Flossing
The greater occipital nerve is frequently implicated in CGH, particularly in traumatic whiplash cases. Recent research has shown that “The obliquus capitis inferior remains relatively immobile during traumatic events, like whiplash injuries, placing strain as a tethering point on the greater occipital nerve.” (23). This trauma may lead to irritation, inflammation, and loss of neuroplasticity, i.e., adhesions.
In patients with cervicogenic tension-type headaches, the combination of neural mobilization and soft tissue techniques induces a significant improvement in pain and function. (24) Here’s how that’s performed:
Adhesions along the course of the nerve may develop secondary to any traumatic or inflammatory process. "Nerve flossing" may help release adhesions and restore normal neurodynamics. Begin with the patient lying supine, headpiece slightly extended. Have the patient bring their fingertips to their clavicles. Firmly grasp the patient's head and move their neck into full flexion while maintaining a chin tuck. Ask the patient to fully extend their arms, wrists, and fingers while you simultaneously move their head and neck into full extension. Return to the start position and slowly repeat ten flossing cycles. Stop if there is a reproduction of pain or neurologic symptoms. To improve available ROM, this maneuver may be preceded contract-relax stretching of the suboccipitals.
3. ADL Advice: Workstation
Routine daily activities involving workstations and cell phones can be potent postural trainers to guarantee a flexor-dominated (forward/ head, forward/shoulder) posture. While manipulation is an effective tool for resolving the symptoms of this postural fault, it’s no match for the cause. Thirty seconds of HVLA three times per week rarely wins the long-term war against eight-plus hours of ongoing postural stress. Lasting improvement necessitates a plan to minimize cumulative trauma.
In addition to equipping our patients with corrective exercises, we must seek to eliminate the habits, hobbies, activities, and postures that perpetuate postural imbalance; and workstations are at the top of that list. Make sure your patients understand the essentials of an ergonomically friendly workstation:
Workstation Ergonomics
Monitors should be visible without leaning or straining, and the top line of the type should be 15 degrees below eye level.
Use audio equipment that keeps you from bending your neck (i.e., Bluetooth, speakerphones, headsets).
Keep your shoulders relaxed, and elbows bent to 90 degrees.
Wrists should not be bent while at the keyboard, and forearms and wrists should not be leaning on a hard edge.
Keep frequently used objects, like your telephone, close to your body to prevent excessive reaching.
Take a 10-second break every 20 minutes. Micro activities include walking, stretching, or moving your head in a "plus sign" fashion.
Periodically, perform the "Brugger relief position" -position your body at a chair's edge, feet pointed outward. Your weight should be on your legs, and your abdomen should be relaxed. Tilt your pelvis forward, lift your sternum, arch your back, drop your arms, and roll out your palms while squeezing your shoulders together. Take a few deep, cleansing breaths.
We’ve broken down the assessment, management, and rehab for cervicogenic headaches. Now, it’s time to ensure that your patients are equipped with the education they need to stay compliant and active in their recovery.
That’s precisely what ChiroUp’s condition-specific reports are designed to do.
Check out a sample of ChiroUp’s Cervicogenic Headache condition report in the link attached.
You can create customizable reports like the one attached for 100+ different conditions in seconds. Have you built a report yet? Visit our Plans & Pricing page to see how you can get started for free.
-
Stovner LJ, Hagen K, Jensen R, Katsarava Z, Lipton RB, Scher AI, Steiner TJ, Zwart JA. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007 Mar;27(3):193-210. Link
Racicki S, Gerwin S, DiClaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. Journal of manual & manipulative therapy. 2013 May 1;21(2):113-24. Link
Nilsson N. A randomized controlled trial of the effect of spinal manipulation in the treatment of cervicogenic headache. Journal of manipulative and physiological therapeutics. 1995 Sep;18(7):435-40. Link
Schoensee SK, Jensen G, Nicholson G, Gossman M, Katholi C. The effect of mobilization on cervical headaches. Journal of Orthopaedic & Sports Physical Therapy. 1995 Apr;21(4):184-96. Link
Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache. Journal of manipulative and physiological therapeutics. 1997 Jun;20(5):326-30. Link
Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D, Emberson J, Marschner I, Richardson C. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine. 2002 Sep 1;27(17):1835-43. Link
McCrory, Penzlen, Hasselblad, Gray. Duke Evidence Report (2001)
Antonia GC. Efficacy of manual and manipulative therapy in the perception of pain and cervical motion in patients with tension-type headache: a randomized, controlled clinical trial. Journal of chiropractic medicine. 2014 Mar 1;13(1):4-13. Link
Dunning JR, Butts R, Mourad F, Young I, Fernandez-de-las Peñas C, Hagins M, Stanislawski T, Donley J, Buck D, Hooks TR, Cleland JA. Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: a multi-center randomized clinical trial. BMC musculoskeletal disorders. 2016 Dec;17(1):64.
Link
Garcia JD, Arnold S, Tetley K, Voight K, Frank RA. Mobilization and manipulation of the cervical spine in patients with cervicogenic headache: any scientific evidence?. Frontiers in neurology. 2016 Mar 21;7:40. Link
Varatharajan S, Ferguson B, Chrobak K, Shergill Y, Cote P, Wong JJ, Yu H, Shearer HM, Southerst D, Sutton D, Randhawa K. Are non-invasive interventions effective for the management of headaches associated with neck pain? An update of the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. European spine journal. 2016 Jul 1;25(7):1971-99. Link
Malo-Urriés M, Tricás-Moreno JM, Estébanez-de-Miguel E, Hidalgo-García C, Carrasco-Uribarren A, Cabanillas-Barea S. Immediate Effects of Upper Cervical Translatoric Mobilization on Cervical Mobility and Pressure Pain Threshold in Patients With Cervicogenic Headache: A Randomized Controlled Trial. Journal of manipulative and physiological therapeutics. 2017 Nov 1;40(9):649-58. Link
Haas M, Bronfort G, Evans R, Schulz C, Vavrek D, Takaki L, Hanson L, Leininger B, Neradilek MB. Dose-response and efficacy of spinal manipulation for care of cervicogenic headache: a dual-center randomized controlled trial. The Spine Journal. 2018 Oct 1;18(10):1741-54. Link
Malo-Urriés M, Tricás-Moreno JM, Estébanez-de-Miguel E, Hidalgo-García C, Carrasco-Uribarren A, Cabanillas-Barea S. Immediate Effects of Upper Cervical Translatoric Mobilization on Cervical Mobility and Pressure Pain Threshold in Patients With Cervicogenic Headache: A Randomized Controlled Trial. Journal of manipulative and physiological therapeutics. 2017 Nov 1;40(9):649-58. Link
Koes BW, Bouter LM, Van Mameren H, Essers AH, Verstegen GM, Hofhuizen DM, Houben JP, Knipschild PG. Randomised clinical trial of manipulative therapy and physiotherapy for persistent back and neck complaints: results of one year follow up. Bmj. 1992 Mar 7;304(6827):601-5. Link
Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial. Journal of Manipulative and Physiological Therapeutics. 1995;18(3):148-54. Link
Antonaci F, Sjaastad O. Cervicogenic headache: a real headache. Current neurology and neuroscience reports. 2011 Apr 1;11(2):149-55. Link
Biondi DM. Cervicogenic headache: a review of diagnostic and treatment strategies. The Journal of the American Osteopathic Association. 2005 Apr 1;105(4_suppl):16S-22S. Link
Page P., Frank C.C., Lardner R., Assessment and treatment of muscle imbalance: The Janda Approach 2010, Champaign, IL: Human Kinetics.
Falla DL, Jull GA, Hodges PW. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine. 2004 Oct 1;29(19):2108-14. Link
Domenech MA, Sizer PS, Dedrick GS, McGalliard MK, Brismee JM. The deep neck flexor endurance test: normative data scores in healthy adults. PM&R. 2011 Feb 1;3(2):105-10. Link
Harris KD, Heer DM, Roy TC, Santos DM, Whitman JM, Wainner RS. Reliability of a measurement of neck flexor muscle endurance. Physical therapy. 2005 Dec 1;85(12):1349-55. Link
Scherer SS, Schiraldi L, Sapino G, Cambiaso-Daniel J, Gualdi A, Peled ZM, Hagan R, Pietramaggiori G. The Greater Occipital Nerve and Obliquus Capitis Inferior Muscle: Anatomical Interactions and Implications for Occipital Pain Syndromes. Plastic and reconstructive surgery. 2019 Sep 1;144(3):730-6. Link
Ferragut-Garcías A, Plaza-Manzano G, Rodríguez-Blanco C, Velasco-Roldán O, Pecos-Martín D, Oliva-Pascual-Vaca J, Llabrés-Bennasar B, Oliva-Pascual-Vaca Á. Effectiveness of a treatment involving soft tissue techniques and/or neural mobilization techniques in the management of tension-type headache: a randomized controlled trial. Archives of physical medicine and rehabilitation. 2017 Feb 1;98(2):211-9. Link
Fernandez M, Moore C, Tan J, et al. Spinal manipulation for the management of cervicogenic headache: a systematic review and meta-analysis [published online ahead of print, 2020 Jul 4]. Eur J Pain. 2020;10.1002/ejp.1632. doi:10.1002/ejp.1632 Link