
3 Facts Every DC Must Know About Inversion Therapy
Reading time: 3 minutes
Inversion tables are a popular option for many people with LBP. Despite varying prices and results, millions of LBP patients own one, and the global market is expected to grow 5.5% from 2022 to 2030. (1,2)
Inversion table therapy (ITT, Self-gravitation traction, or Vertical traction) is believed to alleviate lower back pain by using gravity to pull apart the lumbar vertebrae. However, inversion therapy is controversial, so providers need the facts. This blog will equip you with evidence-based answers to three essential questions:
Are inversion tables effective?
Who benefits from an inversion table?
Are inversion tables safe?
In less than 3 minutes, you’ll be empowered with answers plus a downloadable infographic to help you relay the facts about inversion therapy.
1. Is inversion therapy effective?

While there is insufficient high-quality inversion table research to definitively answer the question, Does inversion therapy help low back pain?; the existing literature suggests that inversion therapy does provide relief for many LBP patients. (3-10)
Few studies have examined the inversion therapy benefits for a specific structural LBP diagnosis; however, three papers answered the question: Does inversion therapy help bulging discs and sciatica?
[In 85 patients with lumbar disc protrusions, inversion therapy produced] improvements in the VAS, Roland Morris, and Oswestry Disease indices. Also, the 2-year surgery rate in the inversion participants (21%) was significantly lower than in the matched control group (39%). (9)
[In 24 patients with single-level disc protrusion and radiculopathy who were awaiting surgery,] an inversion device resulted in a significant reduction in the need for surgery. Surgery was avoided in 76.9% in the inversion group, whereas it was averted in only 22.2% in the control group. (10)
[In lumbar radiculopathy patients,] inversion therapy may have a positive effect on pain relief if added to [standard care]. (8)
These small studies suggest that in disc-induced sciatica patients, inversion therapy might decrease the need for surgery by 54-77%. So why don’t all chiropractors recommend inversion therapy?
Based upon informal show-of-hands classroom surveys of thousands of participants, most practicing chiropractors do not appreciate the benefits of inversion therapy, despite research showing that it works.
Why? Because we’ve all heard countless patient histories detailing strategies (like inversion therapy) that didn’t resolve the presenting complaint - since if something worked, the patient would probably not need to be in our office! Essentially, we spend our day listening to stories about failed strategies… as does every other provider, including PCPs. This leads to incorrectly biased opinions about “what works.”
In the same way that many chiropractors don't believe that inversion tables are effective, PCPs have the same skewed and incorrect perception of chiropractic care, despite abundant high-quality research proving that what you and I deliver is the BEST option for managing LBP and many other spine-related issues.
So you’ll probably agree it's time for some PCP attitude adjustments! Can you imagine a world where every PCP learned about every success story in your office? …A world where chiropractic spinal manipulation was endorsed by not only every clinical practice guideline but also by every PCP!
The good news is that you and I have a tool to help make that happen. It’s called a PCP Release Synopsis, and ChiroUp can help you deliver that crucial report to every patient's PCP with a couple of mouse clicks. You won't believe how crazy simple it is to change attitudes and change referral patterns. Click here to start changing your world today!
2. Which patients benefit from inversion therapy traction?

Several studies, including one systematic review (12), have found that various forms of lumbar traction can benefit LBP when combined with other therapies. (14-21)
Currently, there is no consensus on the ideal patient selection for formal in-office lumbar traction, much less defined criteria for home inversion therapy. Some authors have suggested that providers may “recognize certain clinical patterns that allow them to [effectively] match patients’ symptomatic presentations to specific traction strategies.” (18,22)
The following formal lumbar traction research may be extrapolated to help predict the utility of home inversion therapy.
A clinical prediction rule identified five predictors of lumbar disc patients who may benefit from traction. The presence of three or more of the following predictors more than doubles the likelihood of “greatly improving” with lumbar traction (response increases from 23.3% to 48.7%). (23)
Sudden onset of symptoms
Short duration of symptoms
No segmental hypomobility
Limited lumbar extension
Low fear-avoidance beliefs
Fritz et al. (24) identified four clinical factors that might help predict the appropriateness of traction:
Symptoms extend distal to the buttock
Signs of nerve root compression
Peripheralization with extension
Positive well leg raise
Other authors have suggested that the subgroup of patients presenting signs and symptoms of nerve root compression and unresponsive to movements centralizing symptoms may benefit from lumbar traction. (8) *ChiroUp subscribers can learn more about centralizing symptoms via directional preference testing here.
Bonus - Off Label use? A few studies have suggested that inversion therapy may be useful for eliminating kidney stone fragments.
Inversion-table treatment is a safe and valuable adjunct in assisting passage of lower pole renal stone fragments after [extracorporeal shock wave lithotripsy] (25)
Percussion, diuresis, and inversion therapy may be safe and effective therapies to assist clearance of lower pole kidney stone fragments following shock wave lithotripsy. (26)
3. Is Inversion therapy safe?

Perhaps the most important question concerns the safety of inversion tables, specifically, Can inversion therapy hurt you? According to a 2022 article in Disability and Rehabilitation (7), inversion table therapy (ITT) is not without risk:
“The US Food and Drug Administration Medical Device Reporting Events Database lists 10 adverse ITT events between 2012 and early 2022. Most of these were not serious, however, there were two incidents of spinal cord injury, one documented with fractures requiring surgery. There was also a third case that resulted in mortality due to brain injury [27].”
“The more serious injuries have been related to failure of the ankle grasping mechanisms resulting in direct trauma to the head and neck [27].
“The physiological effects of being inverted may raise intraocular pressure and consequently aggravate glaucoma. Other ocular injuries such as central vein occlusion and retinal detachment have also been associated with ITT [28,29].”
“Furthermore, a vagotonic effect has been seen on the heart during inversion which resolves when no longer inverted [30].”
Earlier research from the International Journal of Sports Medicine (31) explained a potential mechanism for cardiovascular and cerebrovascular issues:
“Inversion significantly increased heart rate, systolic and diastolic blood pressure, systemic vascular resistance, and left ventricular wall stress. Inversion also resulted in a significant decrease in cardiac output and ejection fraction. Thus inversion produces an increase in [ventricular] afterload and myocardial oxygen demand concomitantly with a decrease in global systolic function, and may be contraindicated in patients with cardiovascular disease.”
Many manufacturers relay the following widely accepted contraindications for inversion therapy (31):
Glaucoma
Retinal detachment
Uncontrolled hypertension
Heart or vascular problems, including an elevated risk of stroke
Severe osteoporosis
Hiiatal hernia
Pregnancy
Obesity
Some legal liability disclaimers have grown to include a broader variety of issues (31):
“Any eye, ear, or balance condition”
“Any condition of the heart or circulatory system”
And ironically, “Any bone, skeletal or spinal cord condition”
Bottom line: Should you recommend home inversion therapy?
That depends. In patients without significant contraindications, inversion therapy may be a safe and effective adjunct, especially for traction-friendly conditions like disc lesions or degeneration. However, patients need to be appropriately screened and understand the risks.
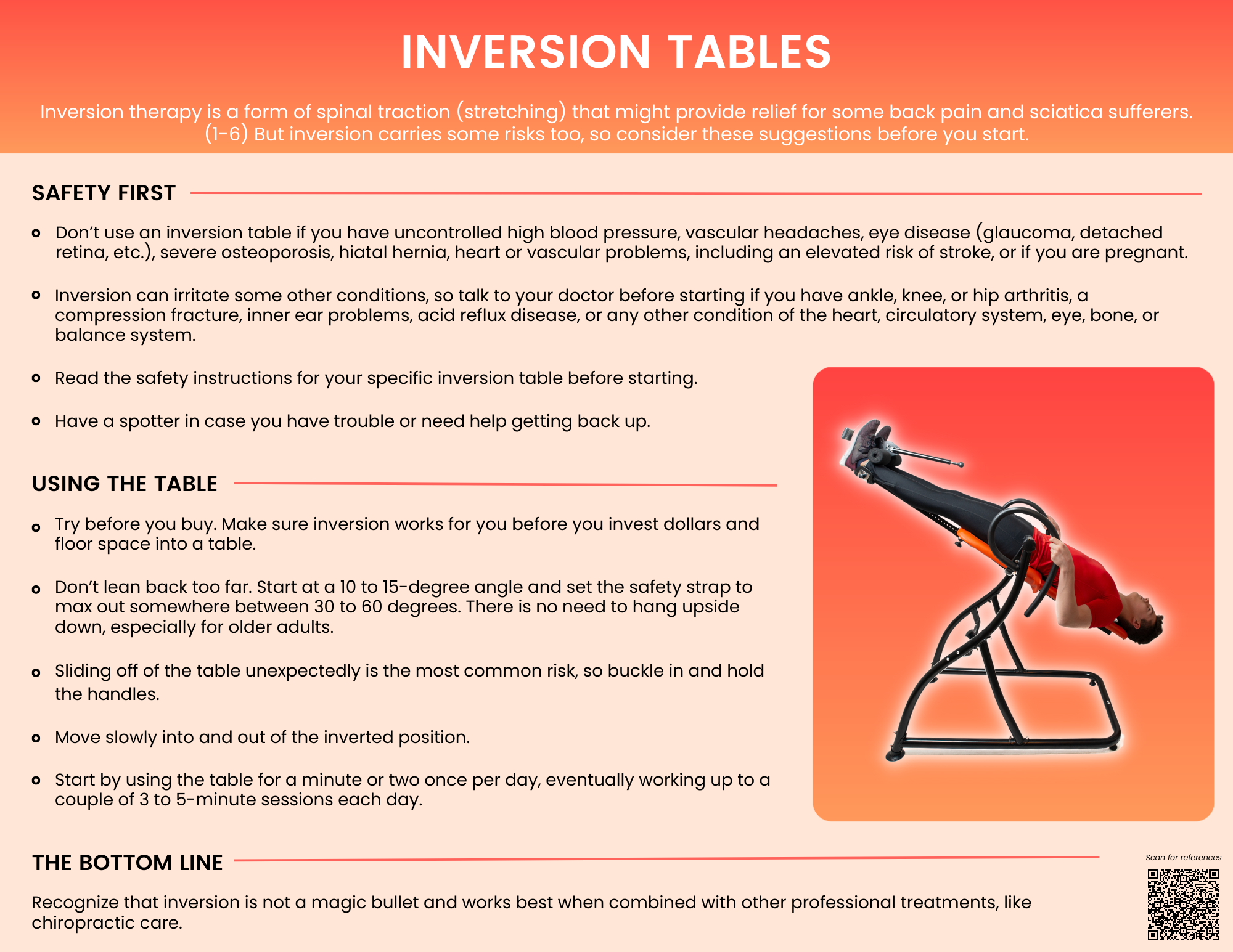
Fortunately, your ChiroUp team has created the following Inversion Therapy infographic to help you relay the facts. Subscribers can download the infographic by visiting the Forms Library and searching “Inversion.”
Elevate your practice and advance our profession by using PCP initial & release reports. ChiroUp is here to make it effortless for you. Get started today with our FREE trial and experience the transformative impact firsthand. Join the 2,500 DCs that are revolutionizing chiropractic care!
-
1. Fact.MR Inversion Table Market Forecast. Accessed on 4/27/23 from Link
2. DataIntelo. Global Inversion Tables Market by Type (Manual Type, Motorized Type), By Application (Household, Gym, Hospital, Others) And By Region (North America, Latin America, Europe, Asia Pacific and Middle East & Africa), Forecast From 2022 To 2030. Accessed on 4/27/23 from Link
3.Güevenol K, Tüzün Ç, Peker Ö, Göktay Y. A comparison of inverted spinal traction and conventional traction in the treatment of lumbar disc herniations. Physiotherapy theory and practice. 2000 Jan 1;16(3):151-60. Link
4. Kassay A, Soliman MA, Jhawar BS. Recommendations for inversion table therapy. Disability and Rehabilitation. 2022 Nov 28:1-4. Link
5. Kane MD, Karl RD, Swain JH. Effects of gravity-facilitated traction on intervertebral dimensions of the lumbar spine. Journal of Orthopaedic & Sports Physical Therapy. 1985 Apr;6(5):281-8. Link
6. Mendelow AD, Gregson BA, Mitchell P, Schofield I, Prasad M, Wynne-Jones G, Kamat A, Patterson M, Rowell L, Hargreaves G. Lumbar disc disease: the effect of inversion on clinical symptoms and a comparison of the rate of surgery after inversion therapy with the rate of surgery in neurosurgery controls. Journal of Physical Therapy Science. 2021;33(11):801-8. Link
7. Kassay A, Soliman MA, Jhawar BS. Recommendations for inversion table therapy. Disability and Rehabilitation. 2022 Nov 28:1-4. Link
8. Vanti C, Turone L, Panizzolo A, Guccione AA, Bertozzi L, Pillastrini P. Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother. 2021 Mar 15;11(1):7. doi: 10.1186/s40945-021-00102-5. PMID: 33715638; PMCID: PMC7958699.
9. Mendelow AD, Gregson BA, Mitchell P, Schofield I, Prasad M, Wynne-Jones G, Kamat A, Patterson M, Rowell L, Hargreaves G. Lumbar disc disease: the effect of inversion on clinical symptoms and a comparison of the rate of surgery after inversion therapy with the rate of surgery in neurosurgery controls. Journal of Physical Therapy Science. 2021;33(11):801-8. Link
10. Prasad KM, Gregson BA, Hargreaves G, Byrnes T, Winburn P, Mendelow AD. Inversion therapy in patients with pure single level lumbar discogenic disease: a pilot randomized trial. Disability and rehabilitation. 2012 Aug 1;34(17):1473-80. Link
11. Kim JD, Oh HW, Lee JH, Cha JY, Ko IG, Jee YS. The effect of inversion traction on pain sensation, lumbar flexibility and trunk muscles strength in patients with chronic low back pain. Isokinetics and Exercise Science. 2013 Jan 1;21(3):237-46. Link
12. Vanti C, Panizzolo A, Turone L, Guccione AA, Violante FS, Pillastrini P, Bertozzi L. Effectiveness of Mechanical Traction for Lumbar Radiculopathy: A Systematic Review and Meta-analysis. Physical Therapy. 2020 Dec 31. Link
14. Fritz JM, Lindsay W, Matheson JW, Brennan GP, Hunter SJ, Moffit SD, Swalberg A, Rodriquez Is there a subgroup of patients with low back pain likely to benefit from mechanical traction?: Results of a randomized clinical trial and subgrouping analysis. Spine. 2007 Dec 15;32(26):E793-800. Link
15. Kim JD, Oh HW, Lee JH, Cha JY, Ko IG, Jee YS. The effect of inversion traction on pain sensation, lumbar flexibility and trunk muscles strength in patients with chronic low back pain. Isokinetics and Exercise Science. 2013 Jan 1;21(3):237-46. Link
16. Simmerman SM, Sizer PS, Dedrick GS, Apte GG, Brismée JM. Immediate changes in spinal height and pain after aquatic vertical traction in patients with persistent low back symptoms: a crossover clinical trial. PM&R. 2011 May 1;3(5):447-57. Link
17. Diab AA, Moustafa IM. The efficacy of lumbar extension traction for sagittal alignment in mechanical low back pain: a randomized trial. Journal of back and musculoskeletal rehabilitation. 2013 Jan 1;26(2):213-20. Link
18. Alrwaily M, Almutiri M, Schneider M. Assessment of variability in traction interventions for patients with low back pain: a systematic review. Chiropractic & manual therapies. 2018 Dec 1;26(1):35. Link
19. Asiri F, Tedla JS, Alshahrani MD, Ahmed I, Reddy RS, Gular K. Effects of patient-specific three-dimensional lumbar traction on pain and functional disability in patients with lumbar intervertebral disc prolapse. Nigerian Journal of Clinical Practice. 2020 Apr 1;23(4):498. Link
20. Vanti C, Panizzolo A, Turone L, Guccione AA, Violante FS, Pillastrini P, Bertozzi L. Effectiveness of Mechanical Traction for Lumbar Radiculopathy: A Systematic Review and Meta-analysis. Physical Therapy. 2020 Dec 31. Link
21. Tanabe H, Akai M, Doi T, Arai S, Fujino K, Hayashi K. Immediate effect of mechanical lumbar traction in patients with chronic low back pain: A crossover, repeated measures, randomized controlled trial. Journal of Orthopaedic Science. 2021 Mar 27. Link
22. Madson TJ, Hollman JH. Lumbar traction for managing low back pain: a survey of physical therapists in the United States. journal of orthopaedic & sports physical therapy. 2015 Aug;45(8):586-95. Link
23. Hirayama K, Tsushima E, Arihara H, Omi Y. Developing a clinical prediction rule to identify patients with lumbar disc herniation who demonstrate short-term improvement with mechanical lumbar traction. Physical therapy research. 2019:E9973. Link
24. Fritz JM, Lindsay W, Matheson JW, Brennan GP, Hunter SJ, Moffit SD, Swalberg A, Rodriquez B. Is there a subgroup of patients with low back pain likely to benefit from mechanical traction?: Results of a randomized clinical trial and subgrouping analysis. Spine. 2007 Dec 15;32(26):E793-800.
25. Ahmed AF, Shalaby E, Maarouf A, Badran Y, Eladl M, Ghobish A. Diuresis and inversion therapy to improve clearance of lower caliceal stones after shock wave lithotripsy: A prospective, randomized, controlled, clinical study. Indian J Urol. 2015 Apr-Jun;31(2):125-31. doi: 10.4103/0970-1591.152813. PMID: 25878414; PMCID: PMC4397549. Link
26. Liu LR, Li QJ, Wei Q, Liu ZH, Xu Y. Percussion, diuresis, and inversion therapy for the passage of lower pole kidney stones following shock wave lithotripsy. Cochrane Database Syst Rev. 2013 Dec 8;(12):CD008569. doi: 10.1002/14651858.CD008569.pub2. PMID: 24318643.
27. Anon. TPLC – total product life cycle; 2022 Accessed 04/27/23 from Link
28. Lerebours VC, Rohl AJ, Shaikh S. Bilateral retinal detachments associated with inversion table therapy. Cureus. 2017;9(3):e1098.
29. LeMarr JD, Golding LA, Adler JG. Intraocular pressure response to inversion. Am J Optom Physiol Opt. 1984; 61(11):679–682.
30. deVries HA, Cailliet R. Vagotonic effect of inversion therapy upon resting neuromuscular tension. Am J Phys Med. 1985; 64(3):119–129.
31. Heng MK, Bai JX, Talian NJ, Vincent WJ, Reese SS, Shaw S, Holland GJ. Changes in cardiovascular function during inversion. Int J Sports Med. 1992 Jan;13(1):69-73. doi: 10.1055/s-2007-1021238. PMID: 1544738.