
Top 10 Clinical Pearls to Differentiate Neurologic Arm Pain
Updated from: 6/28/2018
Neurogenic symptoms in the upper extremity can fool even seasoned clinicians. Evidence-based providers sometimes struggle to differentiate radiculopathy vs. peripheral neuropathy vs. a double crush syndrome…or maybe even something else. To help you nail these diagnoses, ChiroUp has compiled our top 10 tips, including a short nerve tension test tutorial video, and two downloadable diagnostic infographics.
1. Nerve Tension Testing
When assessing sciatica, you ALWAYS perform a straight leg raise, so why wouldn’t you apply the same logic when evaluating upper extremity complaints? Check out this quick nerve tension test tutorial video to review three simple nerve tension tests to help you differentiate upper extremity neurogenic complaints:
Ulnar nerve tension test
Median nerve tension test
Radial Nerve tension test
2. Disc Degeneration vs Disc Herniation
Although generalizations can be dicey since not all conditions adhere to their Merck Manual description, radiculopathy in a patient under age 50 is most likely from disc lesions, while radiculopathy in a patient over age 50 is more likely from degenerative encroachment. (2)
Deeper dive: Want to see how a spinal disc degenerates? Check out this video of the degenerative cascade. (Note: this video illustrates lumbar degeneration; however, the cervical process shares many similarities.)
3. TOS vs Cervical Radiculopathy
Radicular complaints from cervical disc lesions and degeneration most commonly follow a C6 or C7 nerve distribution. In fact, 90% of disc lesions occur at C5/6 (C6 nerve root) or C6/7 (C7 nerve root). (3-5) However, symptoms of TOS follow an ulnar nerve distribution, i.e., C8 or T1, in 90% of cases. (6,7)
Deeper dive: Check out this recent ChiroUp Podcast on What is Thoracic Outlet Syndrome?

4. Shoulder Abduction Sign
Having a patient hold their arm overhead, i.e., Shoulder abduction sign, can help differentiate cervical radiculopathy from TOS. Patients with cervical radiculopathy will find relief in this position, while those with TOS will likely experience worsening symptoms.

5. Testing the LOAF Muscles of the Hand
The ulnar nerve innervates all intrinsic hand muscles except the lateral two lumbricals, opponens pollicis, abductor pollicis, and flexor pollicis brevis, which are innervated by C8 and T1 via the median nerve. (8) Clinicians can differentiate ulnar nerve radiculopathy, i.e., cubital tunnel syndrome, from C8–T1 radiculopathy by examining the (LOAF) hand muscles via pinch grip strength. (8)

Deeper Dive: Even Experts need help with this differentiation. The above-referenced Global Spine Journal study concluded:
“Although all 24 participants considered themselves to be experienced cervical spine surgeons, this study reveals inadequate knowledge regarding the clinical manifestations of C8–T1 radiculopathies and cubital tunnel syndrome.” (8)
Check out this previous ChiroUp blog on 3 Essential Skills for Resolving Cubital Tunnel Syndrome.
6. Differentiating Nerve Irritation vs Compression
Sensory disturbances, including radiculopathy, can occur from simple irritation or inflammation of a nerve; however, motor or reflex loss generally signifies a true compression or more significant pathologic process – that almost always deserves a more substantial response.
The patient often must perform MULTIPLE repetitions before a motor weakness is uncovered. i.e., observing a single heel raise maneuver will catch fewer S1 deficits than watching what happens on the 10th repetition.
7. Bilateral Carpal Tunnel Syndrome
Bilateral carpal tunnel syndrome is unlikely and should suggest central cord involvement until disproven by MRI. (1)
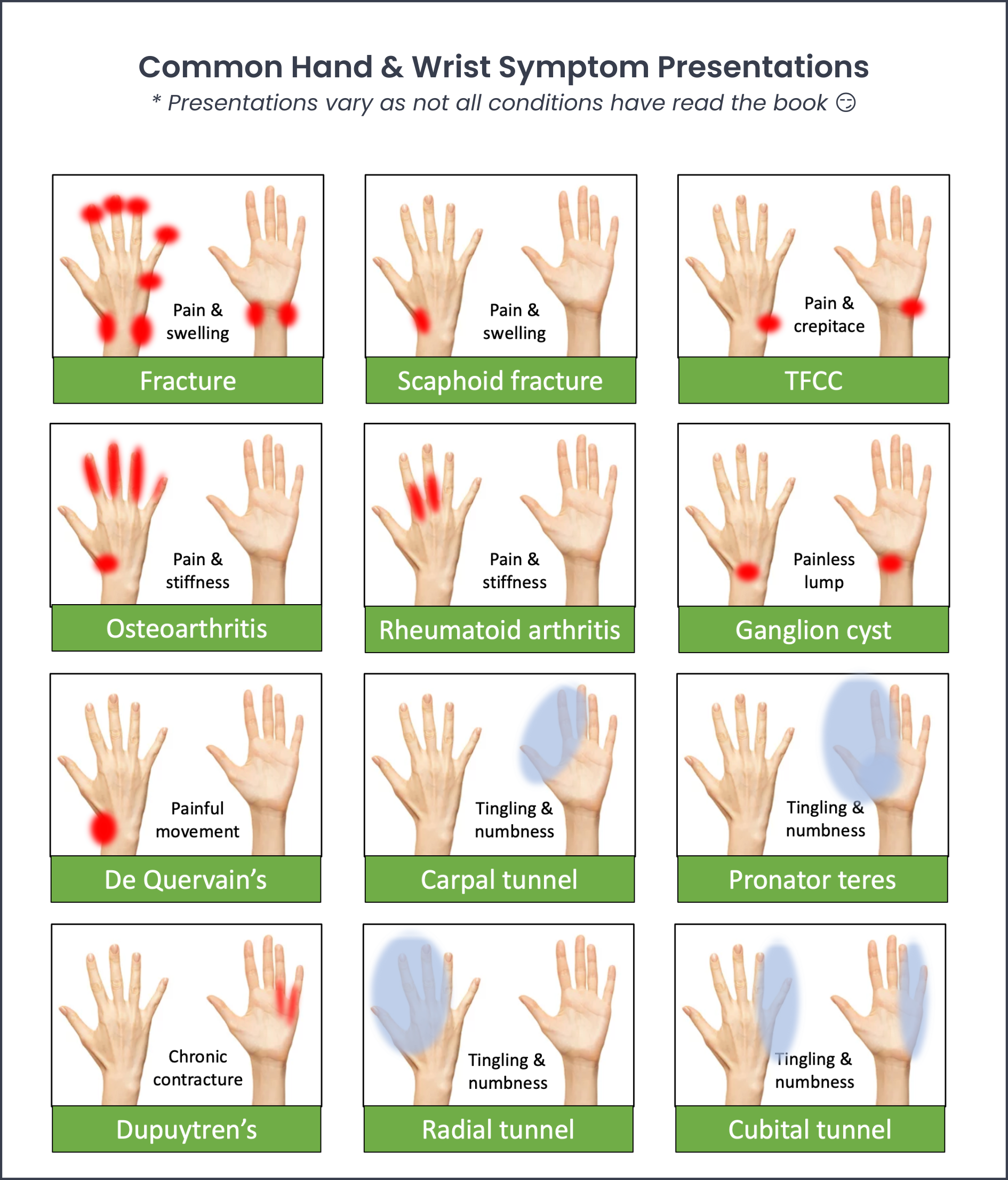
Deeper Dive: Review this Chiropractic Hand & Wrist Exam tutorial video to help you quickly differentiate the most common hand and wrist complaints.
8. CTS vs. Pronator Teres Syndrome
Pronator syndrome is the second most frequent cause of median nerve compression (9.2% of all cases). (9). This condition occurs from entrapment of the median nerve by the pronator teres muscle. Nocturnal exacerbations are common in carpal tunnel syndrome but notably absent in pronator syndrome. Pronator syndrome is the likely diagnosis when symptoms are reproduced within 30 seconds of applying deep sustained compression over the pronator muscle, i.e., Pronator compression test. (10)
Deeper dive: ChiroUp subscribers can visit the Clinical Skills tab to review the Pronator Compression test (or any of the other hundreds of evaluations, treatments, or exercises).

9. Radial Tunnel Syndrome vs. Lateral Epicondylitis
Radial tunnel syndrome commonly mimics or coexists with lateral epicondylitis. Up to 10% of patients diagnosed with lateral epicondylitis actually have radial tunnel syndrome. Nocturnal pain is more common in radial tunnel patients than in those with lateral epicondylitis. Most notably, the peak area of tenderness for radial tunnel syndrome is four finger breaths distal to the lateral epicondyle, i.e., Radial tunnel compression test. (11)
Deeper Dive: Review this Radial Tunnel Syndrome tutorial video, or check out the Radial Tunnel Syndrome blog, including this helpful chart to differentiate RTS vs. Lateral epicondylopathy.

10. Shoulder vs Neck: The Arm Squeeze Test
A simple 2-second evaluation called the Arm Squeeze Test can help differentiate between a shoulder vs. a cervical complaint. In short, compressing the affected arm will exacerbate radicular symptoms via compression of hypersensitized nerves. Arm compression will not exacerbate pain that originates from shoulder dysfunction, i.e., rotator cuff impingement.
In a study of over 1500 patients with arm pain, the Arm Squeeze test showed very high sensitivity (97%), specificity (>91%), and inter/ intraobserver reliability. (12)

Wow, that's a simple but useful test... want something else that’s simple and useful?
Give us two minutes of your time, and we’ll show you how your clinic can leverage resources that other top providers are using.
-
Kim HJ, Tetreault LA, Massicotte EM, Arnold PM, Skelly AC, Brodt ED, Riew KD. Differential diagnosis for cervical spondylotic myelopathy: literature review. Spine. 2013 Oct 15;38(22 Suppl 1):S78-88.
DeLisa JA, Gans BM, Walsh, NE, Physical Medicine and Rehabilitation: Principles and Practice, Volume 1. Wolters Kluwer Health
Constantoyannis C, Konstantinou D, Kourtopoulos H, Papadakis N: Intermittent cervical traction for cervical radiculopathy caused by large-volume herniated disks. J Manipulative Physiol Ther. 2002, 25(3):188-92.
Kramer J. Intervertebral Disk Diseases. Causes, Diagnosis, Treatment and Prophylaxis.
George Thieme Verlag, Stuttgart Year Book, Medical Publishers Inc; 1981.
Wheeless’ Textbook of Orthopaedics. wheelessonline.com
Chang AK. et. al. Thoracic Outlet Syndrome in Emergency Medicine Clinical Presentation. Medscape.com Accessed 6/23/18 at https://emedicine.medscape.com/article/760477-clinical
Stoker GE, Kim HJ, Riew KD. Differentiating C8–T1 Radiculopathy from Ulnar Neuropathy: A Survey of 24 Spine Surgeons. Global Spine Journal. 2014;4(1):1-6.
Gessini L, Jandolo B, Pietrangeli A. Entrapment neuropathies of the median nerve at and above the elbow. Surg Neurol. 1983;19:112-116.
Gainor BJ. The pronator compression test revisited. A forgotten physical sign. Orthop Rev. 1990;19:888-892.
Spinner M, Spinner RJ. Management of nerve compression lesions of the upper extremity. In: Management of Peripheral Nerve Problems, 2nd ed. 1998, Philadelphia, WB Saunders, pp. 501-533.
Gumina S, Carbone S, Albino P et al. Arm squeeze test: a new clinical test to distinguish neck from shoulder pain. European Spine Journal 2013; 22: 1558-63.